


Introduction: Hypomethylating agents (HMAs) are used as induction therapy for patients with acute myeloid leukemia (AML) who are ineligible for intensive chemotherapy. HMA therapy is frequently initiated in the hospital and some patients remain hospitalized through the initiation of cycle 2 (C2). Clinicians are often faced with the decision to administer C2 while the patient is still hospitalized, however, there is a paucity of prognostic information to guide treatment decisions in this common scenario.
Methods: We conducted a retrospective review of patients diagnosed with treatment naïve, de novo and secondary AML who were ineligible for induction chemotherapy (at the discretion of the treating physician based on advanced age, comorbidities, or other reasons) at a single, tertiary, referral center. Patients were included if they received induction therapy with an HMA, including azacitidine and decitabine between 7/1/2008 and 7/1/2018. Exclusion criteria included receipt of intensive induction chemotherapy and inadequate electronic medical documentation. Patients were divided into four groups: patients who were discharged after completion of C1 and received C2 as an outpatient (discharged after C1), patients who received C1 and C2 during the same hospitalization (C1-C2 continuous hospitalization), those who received one total cycle (C1 only), and patients who received C1 as an outpatient (C1 outpatient). The groups were analyzed separately for the primary outcome of overall survival (OS), calculated by Kaplan Meier analysis.
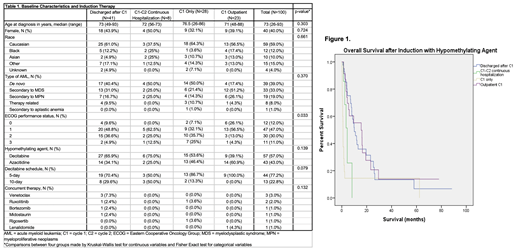
Results: Out of 105 patients identified who received an HMA, 100 patients were identified who met inclusion/exclusion criteria and their baseline characteristics are shown in Table 1. Most patients had de novo AML (39.0%), although 33.0% and 19.0% of patients had AML secondary to myelodysplastic syndrome (MDS) and myeloproliferative neoplasm (MPN), respectively. Additionally, 8 patients (8.0%) had therapy related AML. The majority of patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 1 or 2 at induction. Patients who received C1 as an outpatient had a significantly better performance status than those who did not (p= 0.033) Decitabine was the most common HMA (57.0%) administered and was most often on 5-day schedule. Eight patients (8.0%) were continually hospitalized until C2, 5 because of active medical issues (most often fevers requiring intravenous antibiotics), 2 had physical debility precluding discharge home, and 1 was receiving intrathecal chemotherapy twice weekly for central nervous system involvement of AML.
The median OS was 15.6 months (95% CI 2.66-28.6) in patients who received C1 outpatient, 10 months (95% CI 6.67-13.43) in patients discharged after C1, 4 months (95% CI 2.40-6.40) in the C1-C2 continuous hospitalization group, and 1 month (95% CI 0.61-1.30) in those who only received C1 as shown in Figure 1. Patients discharged after C1 had a significantly longer OS compared to the C1-C2 continuous hospitalization group (p=0.003). There was a trend (p=0.054) towards worse survival in patients who received C1 only compared to patients hospitalized continually from C1-C2.
Conclusions: Continued hospitalization from C1 to C2 of HMA therapy led to an extremely poor median survival of 4 months in this cohort, compared to 10 months in patients who were able to be discharged after C1 and receive C2 as an outpatient. Patients who only received a single cycle of HMA did not have a significantly different survival as compared to patients who were continually hospitalized from C1 to C2.
While this is a small retrospective series, these data suggest that AML patients still requiring hospitalization at time of C2 of HMA therapy should be re-evaluated for alternative therapeutic approaches including hospice given poorer outcomes. Although this grouping selects for patients who are sicker and unable to leave the hospital, there is apparent lack of significant benefit of continued HMA therapy in the majority of patients while inpatient. The impact on hospital length of stay, unnecessary utilization of healthcare resources, and patient's quality of life should also be considered in these cases. Prospective identification of these patients with a poorer prognosis could lead to better alternatives for therapeutic approaches.
Kremyanskaya:Incyte, Celgene, Constellation, Protagonist.: Research Funding; La Jolla: Consultancy. Navada:Onconova Therapeutics Inc: Research Funding. Mascarenhas:Merus: Research Funding; Pharmaessentia: Consultancy, Membership on an entity's Board of Directors or advisory committees; Merck: Research Funding; Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Incyte: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Research Funding; Promedior: Research Funding; Roche: Consultancy, Research Funding; Janssen: Research Funding; CTI Biopharma: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding.
This icon denotes a clinically relevant abstract

