

Introduction
Venous thromboembolism (VTE) and atrial fibrillation are thrombotic disorders resulting in significant morbidity and mortality, if left untreated. In Canada, 45,000 people, or 1-2 cases per 1000 people, per year will experience an acute VTE, and it is estimated that 200,000 Canadians have atrial fibrillation. The treatment of VTE and atrial fibrillation often includes the use of anticoagulants.
Patients on anticoagulation may need interruption of treatment for surgeries and procedures. To evaluate differences in perioperative anticoagulation management strategies we conducted a systematic review of the peri-operative clinical practice guidelines for anticoagulants.
Methods
A protocol using the Preferred Reporting Items for Systematic review and Meta-analysis Protocols (PRISMA-P) was developed. Relevant primary clinical practice guidelines were identified using MEDLINE, EMBASE, and guideline-specific databases. All guidelines from the preceding 20 years up to January 11, 2019 were screened. Eligible manuscripts were reviewed by two independent reviewers. Data abstraction was independently completed in duplicate for included guidances and categorized according to thrombotic risks and bleeding risks. Guidances on emergency surgeries were not included for the purposes of this review. Information on anticoagulation interruption, bridging regimens, laboratory testing, and reversal strategies were collected.
Results
Eight guidelines met inclusion criteria and 6 contained sufficient information for peri-operative management of anticoagulants. One guideline focused on patients presenting with bleeding events and restated the same peri-operative guidelines as had been published a year prior by the same group, and was excluded. Another guideline only addressed emergency surgeries and was also excluded from this review. The majority of the guidelines had similar definitions of risk factors for venous and arterial thrombotic events (see table 1). There were no conflicting guidance recommendations identified, but there were differences in the component of peri-operative management addressed by each guideline, ie bridging, reversal agents, laboratory tests. The levels of evidence used to develop recommendations varied between guidelines. All guidelines provided recommendations on warfarin and low molecular weight heparins (LMWH) management and only one guideline provided suggestions for direct oral anticoagulants (DOACs).
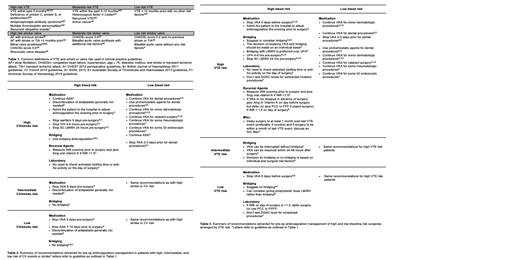
The findings for perioperative anticoagulation management for patients with atrial fibrillation and VTE are presented in Tables 2 and 3, respectively. For high bleeding risk surgeries, most guidelines cited similar studies resulting in similar recommendations for interruption of warfarin and bridging in high venous and arterial thrombotic risk patients. In high bleeding risk procedures and low thrombotic risk patients, no bridging is recommended.
For low bleed risk procedures, regardless of thrombotic risk, guidelines recommended for continuation of anticoagulant therapy.
Discussion
This systematic review identified 6 guidelines of non-urgent peri-operative management recommendations of primarily warfarin and LMWH in patients with VTE and atrial fibrillation. While no major discrepancies in the guideline suggestions were noted, the scope of data examined (medication management, bridging, blood tests, reversal of agents) differed amongst the various agencies. The guidelines that were most consistent for recommendations of anticoagulant management and bridging tended to be from hematologic societies.
The only guideline that addressed perioperative management of DOACs was the 2018 ASH guideline on management of VTE which was against measurement of DOAC levels prior to procedures. The lack of thorough guidance for DOACs is likely due to the year of publication of the guidelines examined and paucity of contributing studies. In terms of reversal agents, all clinical practice guidelines except for the ASH guidelines were prior to specific DOAC reversal agents such as idaracizumab.
Future Directions
We anticipate that there will be other guidelines developed that address specifically the use of DOACs in the perioperative setting, as well as their reversal agents.
Shivji:BMS-Pfizer Thrombosis Canada: Other: Fellowship award. Castellucci:BMS: Honoraria; Pfizer: Honoraria; Bayer: Honoraria; LEO Pharma: Honoraria; Sanofi: Honoraria; Aspen: Honoraria; Servier: Honoraria.

