

Background: Sickle cell disease (SCD) is associated with perioperative complications. Red cell transfusion has been recommended in the management of SCD undergoing elective procedure to minimize perioperative complications. The aim of this study was to retrospectively review our experience in the management of children patients with SCD with the Arab-Indian (AI) haplotype undergoing elective and emergency surgery, and to determine blood transfusion requirement and surgery-related perioperative complications.
Patients and Methods: A total number of 173 SCD patients undergoing surgery at Qatif Central Hospital, Qatif, Eastern province, Saudi Arabia was conducted between February 2007 and June 2019. children less than 14 years and above one year were included (111 boys and 62 girls). Patients were divided into two groups: Group A did not receive transfusion and Group B had top-up transfusion. The medical records were reviewed to define the perioperative risks and the postoperative complications in relation to the type of transfusion modality selected.
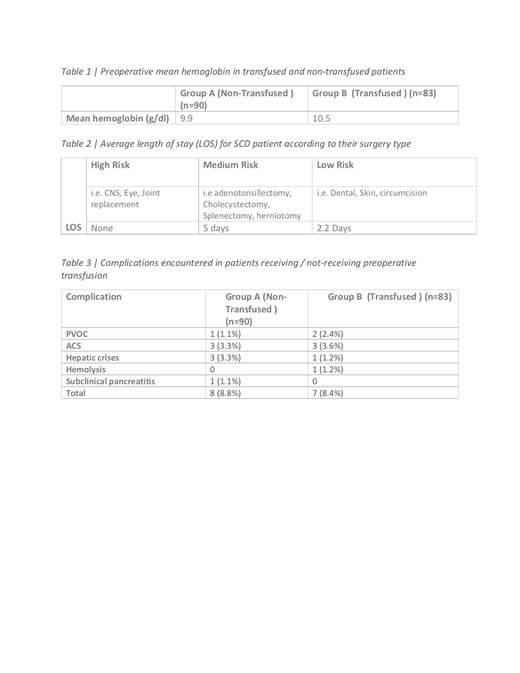
Two surgical procedures were analyzed: a low and medium risk group including laparoscopic cholecystectomy, laparoscopic splenectomy, tonsillectomy, adenotonsillectomy, herniotomy and dental procedure.
Results: eighty-three (n:83) patients (Group A) did not received transfusions (Group B) while . There were 15 (17.2%) postoperative complications; seven (8.4%) occurred in group A patients who did not received transfusion and eight (8.8%) occurred in group B patients who received top-up transfusion. Sickle cell disease-related complications consisted of acute painful vaso-occlusive crises in three patients (3.5%). Six patients (3.9%) had acute chest syndrome, 4 (4.5%) had hepatic crises and one had subclinical pancreatitis. Only one (1.2%) patient in group B (top up) had a mild hemolytic transfusion reaction. Moreover, there was no significant difference in the complications between the transfusion and none transfusion subgroups.
Conclusion: Surgery in SCD patients is safe without a preoperative blood transfusion. Moreover, there was no significant difference in the complications between the transfusion and none transfusion subgroups. To conclude, blood transfusion or exchange blood transfusion should be individualized based on genotype, haplotype and type of surgery.
No relevant conflicts of interest to declare.

