

Introduction
Sickle cell disease (SCD) is an inherited disorder in which pathology is driven by hemoglobin polymerization and red blood cell sickling, leading to chronic anemia, hemolysis, and episodic vaso-occlusion. Anemia affects the brain, kidneys and cardiovascular system, and is associated with neurocognitive dysfunction, silent cerebral infarction, stroke, renal dysfunction, pulmonary hypertension, and mortality. Limited research has been conducted to quantify the economic burden of end organ damage among patients with sickle cell disease in the US.
Methods
Patients with ≥3 nondiagnostic SCD ICD-9/ICD-10 codes within 5 years (Jan 1, 2013-Dec 31, 2017) were identified in the MarketScan® Medicaid claims databases. The first date of SCD diagnosis was the index date. At least three months of continuous enrollment with medical and pharmacy benefits prior to the index date, and at least 1 month of continuous enrollment following the index date were required to be included. Each patient's post-index period was divided into a series of 3-month intervals. For each 3-month interval, patients' entire available claims history (as early as 1/1/2008) was checked to identify four types of end organ damage experienced by SCD patients including stroke (within 1st year and >1 year after an acute stroke event), chronic kidney disease (CKD), end-stage renal disease (ESRD), and pulmonary hypertension (PH). Total healthcare costs (plan paid and patient out-of-pocket payment) and healthcare resource utilization (HRU) information were determined for each 3-month interval. Patient characteristics, HRU, and costs were summarized descriptively by type of end organ damage. Three multivariate generalized linear models with loglink function and gamma error distribution (assuming the cost follows an exponential relationship to the weighted average of covariates) were employed to estimate the relative cost ratios of patients with vs. without end organ damage, controlling for patients' demographic and clinical characteristics. Annualized costs for adult patients with each type of end organ damage were estimated based on the regression results.
Results
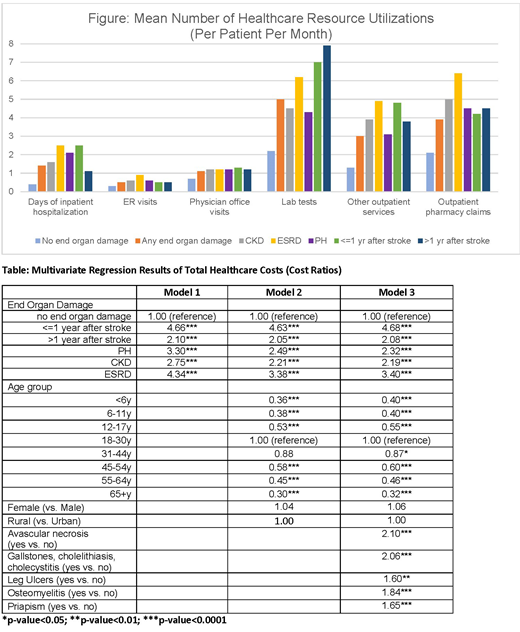
A total of 10,784 patients with SCD on Medicaid were identified. Patients were followed for 3.35 years on average, contributing 152,455 intervals (age ≥18: 42.7%; female: 54.6%; urban: 84.4%). Approximately 20% of the intervals had end organ damage. Patients with end organ damage had more days in hospital, ER visits, outpatient visits, lab tests, and outpatient pharmacy claims per month than patients without organ damage (Figure). The mean (SD) cost per hospitalization for acute stroke was $55,314 ($76, 847). In multivariate regression model 1 (accounting for end organ damage only), patients with any end organ damage had significantly higher costs than those without these conditions. After controlling for patient demographic characteristics (model 2) and additional clinical characteristics (model 3), the results were similar. The costs of SCD patients in the first year after stroke are 4.68 times as high as the costs of patients without any organ damage (2.08 times if >1 yr after stroke; 2.32 times for PH; 2.19 times for CKD; and 3.40 times for ESRD) (Table). The transitional age group (18-30 years) had significantly higher costs than other age groups. Having other SCD complications such as avascular necrosis, gallstones, cholelithiasis, cholecystitis, leg ulcers, osteomyelitis, or priapism also significantly increased the total costs. Based on model 3, after controlling for patient demographics and clinical characteristics, the predicted mean annual costs for adult patients with SCD in the first year after a stroke is $285,816; $127,393 if more than one year after a stroke; $148,174, $135,492, or $209,172 if the patient had PH, CKD or ESRD, respectively. Patients with multiple SCD complications had even higher costs. For example, the predicted mean annual cost for adult patients with CKD and avascular necrosis is $270,513.
Conclusions
Sickle cell disease is associated with substantial economic burden. When patients experience end organ damage such as stroke, renal dysfunction, or cardiopulmonary conditions, this economic burden is significantly elevated. SCD management strategies that can potentially reduce the risks of end organ damage offer both clinical and economic values to patients and society.
Song:Global Blood Therapeutics: Other: Xue Song is an employee of IBM Watson Health, which receives funding from Global Blood Therapeutics to conduct research. Campbell:Cyclerion: Consultancy, Research Funding; Novartis: Research Funding; Global Blood Therapeutics: Consultancy, Research Funding. Cong:Global Blood Therapeutics: Employment, Equity Ownership. Agodoa:Global Blood Therapeutics: Employment, Equity Ownership. Martinez:Global Blood Therapeutics: Other: Diane Martinez is an employee of IBM Watson Health, which receives funding from Global Blood Therapeutics to conduct research. Lew:Global Blood Therapeutics: Other: Carolyn Lew is an employee of IBM Watson Health, which receives funding from Global Blood Therapeutics to conduct research. Black:Global Blood Therapeutics: Other: Danae Black is an employee of IBM Watson Health, which receives funding from Global Blood Therapeutics to conduct research. Varker:Global Blood Therapeutics: Other: Helen Varker is an employee of IBM Watson Health, which receives funding from Global Blood Therapeutics to conduct research. Chan:Global Blood Therapeutics: Other: Chris Chan is an employee of IBM Watson Health, which receives funding from Global Blood Therapeutics to conduct research. Lanzkron:Pfizer: Research Funding; Ironwood: Research Funding; Global Blood Therapeutics: Research Funding; HRSA: Research Funding; NIH: Research Funding; PCORI: Research Funding.

