

Introduction: Standard-of-care (SoC) frontline treatments in Latin America (LATAM) for patients with newly diagnosed multiple myeloma (NDMM) who are transplant ineligible include bortezomib- and thalidomide-based regimens. The uptake of novel MM therapies has been slow in the past decade in LATAM. Recently, the phase 3 ALCYONE study demonstrated that D-VMP significantly improved progression-free survival (PFS) and led to higher rates of deeper responses compared with bortezomib, melphalan, and prednisone (VMP) therapy alone for patients with NDMM who were transplant ineligible (Mateos MV, et al. NEJM. 2018;378[6]:518-528). In this propensity score matching (PSM) analysis, we compared the efficacy of D-VMP with SoC regimens used in LATAM in patients with NDMM who were transplant ineligible.
Methods: Data for the D-VMP cohort were from the randomized, multicenter, open-label, international, phase 3 ALCYONE study, which enrolled patients from 162 sites in 25 countries between February 9, 2015 and July 14, 2016. Patients (N = 706) were randomly assigned to receive 9 cycles of VMP alone (n = 356) or with daratumumab until disease progression (D-VMP; n = 350). Data for the LATAM SoC cohort were from the retrospective, observational Hemato-Oncology Latin America (HOLA) study of patients with selected hematologic malignancies seen in 30 sites across 7 countries in LATAM from January 1, 2008 to December 31, 2015. Patients were required to be ≥18 years of age at MM diagnosis, to have follow-up data for ≥1 year following diagnosis or until death, and to have never received autologous stem-cell transplantation (ASCT). Follow-up continued until the patient's death or December 31, 2016, whichever occurred first.
PSM was conducted to adjust for differences in baseline characteristics between the ALCYONE study and the HOLA registry. Several matching algorithms were tested (eg, exact, optimal, and nearest neighbor). The matching method with the lowest average standardized difference was used for further analyses. Considered baseline characteristics included median age (71 vs 64 years), male sex (46% vs 50%), International Staging System (ISS) I-III (20%, 40%, and 41% vs 11%, 19%, 35% and NA=34%), chronic kidney disease (CKD) (1% vs 33%), and hypercalcemia (11% vs 20%). Outcomes of interest were overall survival (OS) and PFS. OS and PFS were compared based on Cox hazard models. The following outcome regressions were conducted: naïve and multivariate regression on matched samples. The latter was the base case, as differences in baseline characteristics might persist after matching.
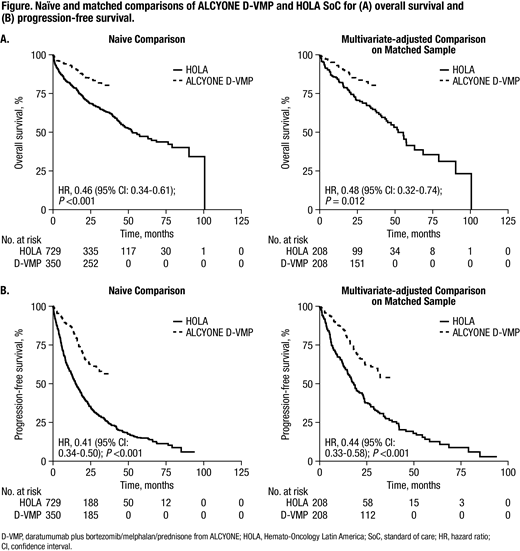
Results: A total of 350 patients from the D-VMP ALCYONE cohort and 729 patients from LATAM in the HOLA cohort were considered for analysis. All D-VMP patients were included; among the HOLA cohort, 478 patients were not missing data for baseline characteristics and were included in the analysis of OS and PFS. The chi-square test showed that baseline characteristics were significantly different between the cohorts. The nearest neighbour PSM with caliper 0.05 was selected for OS and PFS. After matching, the chi-square test demonstrated that baseline characteristics of remaining matched patients were well-balanced (no significant differences in covariates) between D-VMP (n = 207) and HOLA (n = 207) in terms of median age (70 vs 70 years), sex (male, 50% vs 47%), ISS I-III (16%, 38%, and 46% vs 22%, 38%, and 40%), CKD (2% vs 3%), and hypercalcemia (16% vs 14%). D-VMP showed statistically significantly better OS and PFS compared with HOLA. The naïve hazard ratio for OS was 0.46 (95% CI: 0.34-0.61) and for PFS was 0.41 (95% CI: 0.34-0.50); the base case hazard ratio for OS was 0.48 (95% CI: 0.32-0.73) and for PFS was 0.44 (95% CI: 0.33-0.58; Figure).
Conclusions: This analysis demonstrated a benefit of D-VMP over SoC treatments in LATAM for OS and PFS. Results should be considered in the context that ALCYONE OS data are immature, and there are potential limitations of temporal bias, measurement bias, and bias due to unobserved confounding factors between the two cohorts.
Hungria:BMS: Consultancy, Honoraria, Speakers Bureau; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; BMS: Consultancy, Honoraria, Speakers Bureau; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Abbvie: Consultancy, Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Abbvie: Consultancy, Membership on an entity's Board of Directors or advisory committees. Martinez-Banos:Celgene, Amgen: Other: Advisory Board. Mateos:GSK: Membership on an entity's Board of Directors or advisory committees; Pharmamar: Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees; EDO: Membership on an entity's Board of Directors or advisory committees; Adaptive: Honoraria; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees. Dimopoulos:Sanofi Oncology: Research Funding. Cavo:Celgene, Janssen, Amgen, BMS, Abbvie, Takeda: Honoraria; Janssen, Celgene: Other: Travel Accommodations; Janssen, Celgene: Speakers Bureau; Janssen, Celgene, Amgen, Abbvie: Consultancy, Membership on an entity's Board of Directors or advisory committees. Heeg:Ingress-Health: Employment. Lam:Janssen: Employment, Equity Ownership. Machnicki:Janssen: Employment, Equity Ownership. He:Janssen: Employment, Equity Ownership. Fernandez:Janssen: Employment, Equity Ownership.

