

Background: Patients with Chronic Lymphocytic Leukemia (CLL) are susceptible to infections due to impaired immunity, from both complications of disease and treatments. Specific treatments such as fludarabine or rituximab are incorporated in chemotherapy regimens for CLL and cause lymphocyte depletion and impaired humoral immunity, resulting in increased risk of fungal infections. The aim of this study is to explore the incidence rates of fungal infections in patients before and after treatment for CLL.
Methods: We identified patients diagnosed with CLL using ICD9 code 204.1X within the Veterans Health Affairs (VHA) between 1999 and 2013, before the availability of novel agents for CLL. Pharmacy records were used to identify treatment of CLL (alemtuzumab, bendamustine, chlorambucil, fludarabine, ofatumumab, pentostatin, and rituximab) as well as anti-fungal agents (amphotericin, caspofungin,fluconazole, flucytosine, itraconazole, ketoconazole, micafungin, posaconazole, and voriconazole). Fungal infections were identified with two strategies, using ICD9 codes alone (candida 112.X; pneumocystis 136.3; coccidiomycosis 114.x; histoplasmosis 115.X; blastomycosis 116.X; aspergillus 117.3; cryptococcus 117.5; opportunistic mycoses 118.X) as well as using ICD9 codes combined with evidence of treatment with an anti-fungal (ICD9+antifungal). Number of infections and incidence rates were categorized as occurring in patients prior to first treatment (pre-treat), or after first treatment (post-treat), or in patients who had never received treatment within the VHA (no-treat). Incidence rate ratio between pre- and post-treatment period was calculated to quantify the magnitude of risk increase in patients who received CLL treatment.
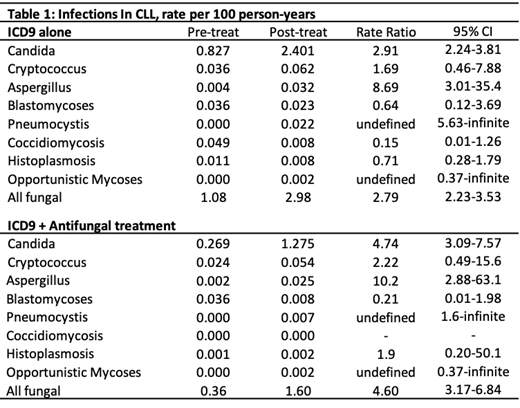
Results: A cohort of 20,023 patients were identified with CLL and followed for a mean of 5.33 years for a total surveillance of 106,772 person-years. Of these patients, 3,726 (18.6%) received treatment for CLL within the VHA. Using ICD9 codes alone, 970 fungal infections were identified and with ICD9+anti-fungal, 415 patients had an infection. With ICD9, the most common infection was candida with 765 infections, followed by aspergillus with 58 and pneumocystis with 39 infections. Rates of infections based on ICD9 were highest in the post-treat group with 2.98 infections per 100 person-years, followed by 1.08 infections per 100 person-years in the pre-treat group and 0.58 infections per 100 person-years in the no-treat group. The most common first treatment was rituximab alone, used in 35.9% of patients, followed by chlorambucil in 31.9%, fludarabine in 20.4%, and bendamustine in 9.9%. In comparison to pre-treat patients, post-treat patients had 2.91 times increased risk of fungal infection (95% confidence interval (CI) 2.24-3.81) determined by ICD9 code and 4.74 times increased risk (95% CI 3.09-7.57) determined by ICD9+antifungal. The rate of candida infection increased 2.9 fold (95% CI 2.24-3.81) with ICD9 and 4.7 fold (95% CI 3.09-7.57) with ICD9+antifungal while aspergillus infections increased 8.7 fold (95% CI 3.01-35.4) with ICD9 and 10.2 fold (95% CI 2.88-63.1) with ICD9+antifungal between post-treat and pre-treat groups.
Conclusions: In this retrospective analysis of CLL patients, treatment for CLL significantly increased the rate of fungal infections, primarily candida and aspergillus. Further study is needed to understand the effect of modern treatments on fungal infections in CLL.
Schoen:Pharmacyclics: Research Funding. Georgantopoulos:Pharmacyclics: Research Funding. Bennett:Pharmacyclics: Research Funding.

