

Abstract
Background: There are well-established prognostic factors for predicting the overall survival (OS) of patients involved by diffuse large B cell lymphoma (DLBCL). These prognostic factors are age, performance status (PS; ECOG score), high serum lactate dehydrogenase level (LDH), advanced disease (Ann Arbor stage: III, IV) and extranodal sites involved (EN). The patients are distributed in different risk groups according to the score obtained and as established by each research group who developed each international index. However, these prognostic indexes do not explore new markers and just readjust the five known variables since 1993 when The International Non-Hodgkin's Lymphoma Prognostic Factors Project was developed. Serum albumin (SA) has been shown to be a prognostic biomarker in DLBCL prior to R-CHOP treatment (Ngo et al. Leuk Lymph 2008). In another study of patients older than 80 years receiving R-miniCHOP treatment, SA ≤3.5 g/dl was the only factor with a significant effect on OS on (Peyrade et al Lancet Oncol 2011). Studies of non-Hodgkin's lymphoma reported that SA <3.0 g/dl was one of the factors predicting early death from aggressive disease treated with ACVBP (Dumontet et al. Br J Haematol 2002). Another study found that SA <3.7 g/dl is an independent prognostic indicator in DLBCL patients treated with R-CHOP (Dalia et al. Ann Hematol 2014).
Aims. The present study evaluates the behavior of IPI, RIPI and NCCN-IPI risk groups obtained from a database of 855 patients involved by DLBCL and explores a cut-off for SA and the addition of it as part of those risk groups.
Methods. Seven databases were obtained from different public and private institutions in the country with patients diagnosed with DLBCL. Creating a unique database with 855 patients. Only 811 patients had serum albumin levels in their record (94.8%). Statistical methods: First, we decided to obtain the SA cut-off through the Received Operating Curve because any study has evaluated this (including sensibility, specificity, likelihood ratio positive and negative). Thus, we evaluated the influence of SA in OS. For that, OS was assed using Kaplan-Meier method (KM) and compared between obtained groups using log rank-test. Subsequently, we add SA score to the different risk prognostic index groups and were assed using KM again. Hazard ratio was evaluated using cox-regression model (CRM).
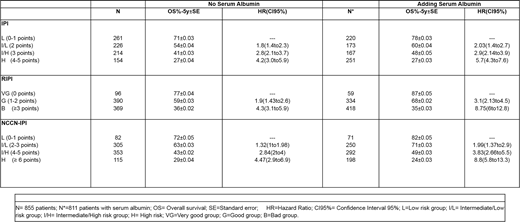
Outcomes. From 2008 to 2016 were included from seven different databases in one, 855 patients of different institutions (publics, academics and privates) in different States. Demographic characteristics: Female,51.46%; Median age was 63 y/o (range: 18-96), ≥ 60, 54.8%; PS, ECOG ≥2,31.1%; EN ≥ 1, 32%; LDH > normal, 52.74%. Type of regimen: Rituximab + anthracycline-based regimen= 75%, anthracycline-based regimen=10.5%, rituximab + CVP= 7%, Other treatments=4.5%, No treatment= 3%. All of them were included as intent-to-analyses. The classical variables were evaluated using the CRM, for IPI and RIPI; age and LDH were evaluated according to the proposed cut-off or ratio respectively in the original paper for NCCN-IPI, confirming that all were significant as predictor factors (p <0.0001). The Area under the curve for SA in relation to OS was 0.70 (CI95% = 0.67 to 0.73, p <0.0001) and the cut-off point was <3.2g / dL. However, we observed that SA had two cut-off points with different predictive value that perfectly differentiated two groups. These points were for low group: 3.2 g / dL to 2.5 g / dL (PPV=68%, NPV= 68.1%) and for very low group: ≤2.4 g/dL (PPV=80% , NPV=60.5%). Then, we evaluated its influence in OS, normal SA was 64% ±0.02 vs low group 34%±0.03 (HR=2.6, CI95%=2to3.5) vs. Very low group 16%±0.04 (HR=4.5, CI95%=3to7). For the addition of SA to IPI, RIPI and NCCN-IPI, we gave a 1 point to Low and 2 points to very low; Then, these points were added to the risk scores of the different IPI, which increased the final scores or not. In Table 1, the percentages of OS of each risk group can be compared before and after adding the points according to the SA score. Where adding SA significantly improves the distribution of risk groups. See table 1.
Conclusion: SA is an important predictive factor of OS in patients involved by DLBCL. Two risk groups can be observed according to the SA level. The addition of SA to the prognostic indexes improves the distribution of patients and the OS percentage at 5 years of follow-up.
Gomez-Almaguer:AbbVie: Consultancy; Novartis: Consultancy.

