Abstract
Introduction: Cardiac dysfunction in thalassemia remains of primary concern. The prevalence of these abnormalities varies in different phenotypic/genotypic groups of thalassemia.
Objective: To describe the difference in cardiac function among Thalassemia Major ™, Thalassemia Intermedia (TI), and Sickle-Thalassemia (ST) patients.
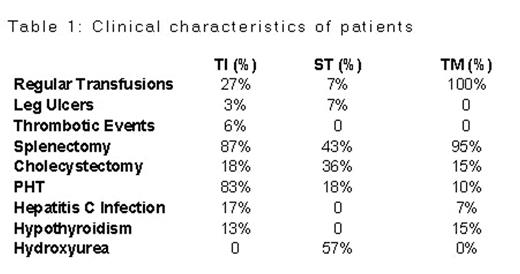
Methods: 66 TM, 41 TI and 17 ST patients were randomly selected from a population of 450 TM,100 TI and 26 ST patients respectively. The patients were interviewed and their charts reviewed and all had an echocardiography. Pulmonary Hypertension (PHT) was defined as Pulmonary Artery Systolic Pressure> 30mmHg.
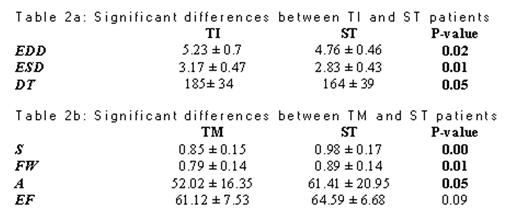
Results: 58.8%, 50% and 41.5% of ST,TM and TI patients respectively were males. Mean age was 24.4 ± 11.6, 19.4 ± 7.6, 19.5 ± 10.9 year old for TI, TM and ST. Tricuspid Regurgitant jet was detected in 47%, 30% and 82% of TI, TM & ST patients respectively. PHT was found in 83%, 18% and 10% of TI, ST, TM patients. Deceleration Time (DT) was significantly longer in TI than in TM and ST, with no significant difference between TM and ST. End diastolic dimension (EDD) was significantly larger in TI than TM and ST (for more details about cardiac parameters refer to tables 2a and 2b). Thrombotic events occurred in 6% of TI patients and in 0 TM and ST patients.
Discussion: PHT is primarily prevalent in TI patients which further supports the notion that a different pathophysiological process leads to this than in TM and ST patients. Moreover these results stress the need for better method of assessment of PHT, because of the limited number of patients in whom a TR jet could be detected. A prolonged DT is one of the earliest sign of diastolic dysfunction in thalassemics. TI patients have revealed themselves to have more impaired diastology by both prolonged DT and Isovolumic relaxation time (IVRT). Splenectomy was performed more in Lebanese TI than that reported in the literature (87% vs 65%), because most of our TI patients were managed as TM. This was before the currently recognized association of splenectomy and PHT and thrombosis. In addition chamber sizes (EDD) was significantly more in TI than both TM and ST patients. This can be attributed to the more profound chronic dilutional volume overload secondary to uncorrected anemia. Finally as is evident TI patients are developing more complications than both TM and ST. Transfusion/ chelation therapy to avoid PHT, diastolic dysfunction and thrombosis in TI patients has been proposed as a solution. If the pathophysiology of these complications is iron-mediated then prophylactic transfusion/ chelation therapy would be more advisable than waiting for them to develop. Especially in view of the morbidity associated with thrombosis, and limitation of exercise tolerance secondary to PHT.
Clinical characteristics of patients
Significant differences between TI and ST patients
Table 2b: Significant differences between TM and ST patients