Abstract
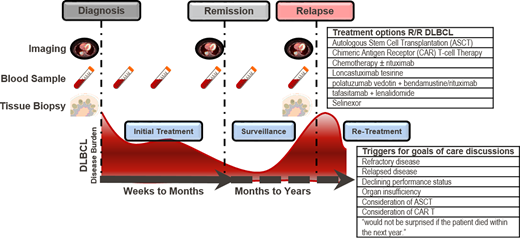
Diffuse large B-cell lymphoma (DLBCL) is the most common lymphoid malignancy worldwide, comprising approximately 30% of all lymphomas. Currently, 50% to 60% of patients diagnosed with DLBCL are alive at 5 years and cured with modern therapy, but about 10% to 15% of patients are refractory to first-line therapy, and an additional 20% to 30% relapse following a complete response. Patients who have relapses beyond 2 years may experience more favorable outcomes and have forms of DLBCL that can be distinguished biologically. Patients who experience early relapse or who have primary refractory disease (less than a complete response or relapse within 3 to 6 months of initial therapy) have worse outcomes. For decades, the standard of care treatment strategy for fit patients with relapsed DLBCL has been salvage therapy with non–cross-resistant combination chemoimmunotherapy regimens followed by high-dose chemotherapy and autologous stem cell transplantation (ASCT) as stem cell rescue for patients with chemosensitive disease. Recent data suggest that certain patients may benefit from chimeric antigen receptor T-cell therapy (CAR T) in the second-line setting. Additional novel therapies exist for patients who are ineligible, who are unable to access these therapies, or who fail ASCT and/or CAR T. Despite the advent of new therapies for DLBCL and improved outcomes, DLBCL remains a life-threatening illness. Thus, it is essential for clinicians to engage in serious illness conversations with their patients. Goals-of-care communication can be improved through skills-based training and has been demonstrated to have an impact on patient experiences.
Learning Objectives
Recognize the therapeutic options available for patients with relapsed/refractory DLBCL
Understand the triggers and process for goals-of-care discussions for patients with relapsed/refractory DLBCL
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common lymphoid malignancy worldwide, comprising approximately 30% of all lymphomas. Currently, 55% to 60% of patients diagnosed with DLBCL are alive at 5 years and cured with modern therapy,1 but approximately 10% to 15% of patients are refractory to first-line therapy, and an additional 20% to 30% relapse following a complete response (CR).2,3 This high-risk DLBCL population constitutes approximately 11 000 individuals annually in the United States.3,4 Evidence suggests that molecular subgroups of DLBCL exhibit significantly different biology, response to standard therapies, and overall survival (OS) based on the cell of origin.5,6 Standard of care first-line therapy for DLBCL has been based on French and US randomized controlled trials (RCTs) completed in 2001 demonstrating that the addition of rituximab (R) to cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) combination chemotherapy improved outcomes over CHOP.7,8 Since then, numerous RCTs have failed to improve upon R-CHOP, including trials targeting patients with poor-risk clinical features by cell-of-origin subtype.9-16 Recently, a double-blind, placebo-controlled, international RCT compared a modified regimen of R-CHOP (pola-R-CHP), in which vincristine was replaced with polatuzumab vedotin as a first-line therapy for patients with intermediate-risk or high-risk DLBCL according to the International Prognostic Index (IPI).17 Progression-free survival (PFS) was significantly higher in the pola-R-CHP group than in the R-CHOP group (stratified hazard ratio [HR], 0.73; 95% CI, 0.57-0.95) with 2-year PFS of 76.7% (95% CI, 72.7-80.8) vs 70.2% (95% CI, 65.8-74.6) for pola-R-CHP and R-CHOP, respectively. The safety profile was similar in the 2 regimens. Changes in the frontline management of DLBCL based upon these results would likely have an impact on therapeutic decisions in the relapse setting (Table 1).
DLBCL prognosis and social determinants of health
The hypothetical stories of Alvin and Wilma are based on real patient scenarios and illustrate some of the key challenges faced by patients with newly diagnosed and relapsed DLBCL. Both patients were diagnosed with stage IV non–germinal center B-cell (GCB) DLBCL with poor prognostic features and an IPI score of 4, placing both in the high-risk category based on similar features. A recent analysis comparing the IPI, revised IPI, and National Comprehensive Cancer Network IPI involved 2124 DLBCL patients treated with R-CHOP or a variant in 1 of 7 multicenter RCTs. These data demonstrated that DLBCL patients in the high-IPI category had 5-year PFS of 45.8% (95% CI, 41.1%-51.0%) and 5-year OS of 53.9% (95% CI, 49.3%-59.1%).18
Although immunohistochemistry (IHC) algorithms have been available for more than a decade and gene expression–based approaches utilizing formalin-fixed paraffin-embedded tissue have been demonstrated to reliably classify DLBCL into biologically and clinically distinct subgroups,19-23 these tests have had little impact on clinical management for patients with newly diagnosed or relapsed DLBCL. Based on gene expression, patients with activated B-cell (ABC) DLBCL (the majority of non-GCB DLBCL) had 5-year PFS of 48% and 5-year OS of 56%, and the cell of origin was identified in this study to have prognostic significance independent of IPI.23 Additional studies found that significant genomic diversity exists within the ABC and GCB subgroups and defined genomic subtypes with prognostic value and potential therapeutic implications.24-26 Currently, there are no clinical assays that can comprehensively and accurately evaluate the genomic profile of DLBCLs with a short turnaround so that this molecular information can be incorporated into clinical workflow and practice.
Additionally, studies indicate that patients diagnosed with DLBCL from rural areas of the United States and that uninsured patients (HR, 1.39; 95% CI, 1.14-1.70) and Medicaid-insured patients (HR, 1.48; 95% CI, 1.23-1.78) with DLBCL had lower survival compared with patients who had private insurance.27,28 Moreover, rural patients, less commonly, had private insurance and high socioeconomic status and were more likely to receive treatment within 14 days of diagnosis.27 Accounting for these social determinants of health is critical in understanding the prognosis for individuals with DLBCL and developing suitable management strategies for first-line therapy and relapse disease. As demonstrated by these patient situations, these sociodemographic factors influence the means to access therapies that can be curative. It is also important to note that even when social factors make therapies more difficult to access, patients can be supported using evidence-based approaches like patient navigation that have a demonstrated impact on outcomes in the first-line and relapse setting.29
Other important studies showed that a shorter diagnosis-to-treatment interval (DTI) was associated with poor prognostic factors. DLBCL patients initiating treatment within 14 days had higher lactate dehydrogenase (LDH) levels, worse Eastern Cooperative Oncology Group Performance Status (ECOG PS), more frequent B symptoms, more bulky disease, and a worse age-adjusted IPI.30 A shorter DTI was associated with worse outcomes in both ABC and GCB subgroups, was prognostic even after adjusting for the IPI, and was a predictor of survival in cohorts across the United States, Europe, Canada, and Japan.30-33 Interestingly, a recent study showed that higher levels of circulating tumor DNA (ctDNA) were associated with shorter DTI and similarly predicted such outcomes, providing a biological pathway for understanding these worse outcomes and a potential biomarker for intervention.31 However, there is limited applicability of ctDNA in routine clinical practice currently.
Conventional management strategies for patients with relapsed DLBCL
For the majority of patients who relapse, this occurs within the first 2 years of initial therapy. Patients who experience early relapse or who have primary refractory disease (less than a CR or a relapse within 3 to 6 months to initial therapy) have worse outcomes.1,34,35 Although patients can be cured with treatments following these early events, most of these patients die from DLBCL. An IPI for relapsed/refractory DLBCL (R/R IPI) was developed using 1234 of 5112 patients treated with frontline immunochemotherapy in the SEAL consortium who experienced progressive disease.36 This study found that time to progression on immunochemotherapy and age at progression were strongly associated with postprogression OS. A prognostic model involving both variables had good concordance in the discovery (0.67) and validation sets (cohort 1, c = 0.64; cohort 2, c = 0.68). A corresponding nomogram is available to aid in estimating prognosis for R/R DLBCL.36 An electronic calculator of the model is also available at https://qxmd.com/calculate/calculator_682/prognosis-calculator-for-relapsed-refractory-dlbcl and as a smartphone app.
Patients who have relapses beyond 2 years may experience more favorable outcomes and have forms of DLBCL that can be distinguished biologically.37 However, despite providing valuable prognostic and predictive information, molecular classification assays including IHC, gene expression profiling, and sequencing panels have faced significant challenges, precluding their transition into routine clinical workflow and practice.21-23,38,39 Even when such biomarkers are available, they have had limited impact on therapeutic decision-making in the relapsed setting. Validated, predictive biomarkers will be an integral component of future personalized medicine strategies for DLBCL.39-41
For decades the standard of care treatment strategy for fit patients with relapsed DLBCL has been salvage therapy with non–cross-resistant combination chemoimmunotherapy regimens followed by high-dose chemotherapy and ASCT as stem cell rescue for patients with chemosensitive disease.42 The pivotal RCTs supporting the modern practice of stem cell transplantation for patients with large B-cell lymphoma include the Parma trial that was conducted in the era before the availability of rituximab and the current World Health Organization lymphoma classification. This study randomized patients with R/R intermediate- to high-grade non-Hodgkin lymphoma with chemosensitivity to proceed with either autologous stem cell transplantation (ASCT) or additional chemotherapy with dexamethasone, high-dose cytarabine, and cisplatin (DHAP). It demonstrated that high-dose chemotherapy followed by ASCT was associated with improved event-free survival (EFS) at 5 years of 46%, vs 12% with DHAP.42 Importantly, the CORAL trial and the LY.12 trial designed to compare DHAP to alternative platinum-containing salvage regimens identified that patients with R/R disease within 12 months of diagnosis and prior exposure to rituximab had poor PFS following salvage therapy.43,44 These findings indicate that the prior demonstrated benefits of ASCT were reduced in the R-CHOP era due to resistance to chemoimmunotherapy, identified by early first-line treatment failure. These poor outcomes associated with early relapse of DLBCL are evident in Alvin's situation. However, ASCT can provide benefits, particularly for patients like Wilma who experience late relapse and have chemosensitive disease. Recent evidence-based guides suggest that ASCT remains a preferred option for patients who experience late relapse.3 Based on the R/R IPI calculator, the predicted 2-year survival from progression for Alvin and Wilma are 34% and 60%, respectively.36
Chimeric antigen receptor T-cell therapy
Current approved chimeric antigen receptor T-cell (CAR T) therapies are genetically engineered cell products targeting the B-cell marker CD19 that are available for patients with R/R DLBCL after at least 2 lines of therapy. These include axicabtagene ciloleucel (axi-cel), tisagenlecleucel (tisa-cel), and lisocabtagene maraleucel (liso-cel). These cellular therapies may differ in their mechanisms of viral transfection, costimulatory domains, and T-cell selection, but each has demonstrated the ability to produce durable remissions in about 30% of patients, including patients who have failed prior ASCT.45-47 Axi-cel uses the CD28 costimulatory domain that interacts with the CD3-zeta activation domain to enhance activation and proliferation of CAR T cells. Tisa-cel and liso-cel have a similar extracellular CD19 single-chain variable fragment attached to a 4-1BB intracellular costimulatory domain connected to a CD3ζ signaling domain. Liso-cel has a distinct manufacturing process involving the separation of CD4 and CD8 T cells after leukapheresis-independent transduction, expansion, and administration to patients at equal target concentrations.
JULIET was an international phase 2 study of tisa-cel in 93 patients with R/R DLBCL who were ineligible for or had disease progression after ASCT.47 The best overall response rate (ORR) was 52% (95% CI, 41%-62%). Grade 3 or 4 adverse events of interest included cytokine release syndrome (CRS) in 22%, neurological events in 12%, and cytopenias lasting more than 28 days in 32%. In a subsequent study of this patient group at a median follow-up of 40.3 months, the ORR was 53% and the PFS at 3 years was 77.8% for patients in CR at 6 months.48 Among 111 patients enrolled in ZUMA-1, axi-cel was manufactured for 110 patients and administered to 101 patients.46 The objective response rate was 82%, and the CR rate was 54%. Grade 3 or higher CRS and neurological events occurred in 13% and 28% of patients, respectively. In a subsequent study of this patient group at a median follow-up of 27 months, the median duration of response for all 101 patients was 11 months and the median duration of response for participants achieving CR was not reached.49 In the TRANSCEND study, 344 patients underwent leukapheresis for the manufacture of CAR T cells, and 269 patients received at least 1 dose of liso-cel.45 Of 256 patients evaluable for response, an objective response was observed in 73% (95% CI, 66.8%–78.0%) and a CR in 53% (95% CI, 46.8%–59.4%). Grade 3 or greater CRS and neurological events occurred in 2% and 10% of patients, respectively. Together these results demonstrate meaningful and durable responses for patients with R/R DLBCL, including those who have failed prior ASCT. This remains a viable alternative for patients who can access these therapies. As described in the patient cases, there may be barriers for certain patient groups, such as those who live in rural areas or who lack insurance coverage for CAR T-cell therapy. Additional measures are necessary to ensure equitable access to potentially curative therapy for all patients.
Common lymphoma-specific bridging therapy administered between leukapheresis and CAR T-cell therapy includes steroids, chemotherapy, targeted therapy, or radiation therapy. The optimal approach for bridging therapy prior to CAR T-cell therapy remains uncertain.3,50-53 Data from 17 academic institutions involved in the US Lymphoma CAR T Consortium showed that bridging therapy was administered to 53% of 298 patients who underwent leukapheresis prior to planned axi-cel. Among these patients 23% received steroids alone, 54% received chemotherapy, 12% received radiation therapy, and 10% received targeted therapy.54 A multivariable analysis in this data set revealed that bridging was associated with inferior OS. However, the need for bridging may be a surrogate for greater disease burden or more aggressive lymphoma. A study by Pinnix and colleagues suggests that radiation may be an effective approach when bridging is required,50 but additional studies are needed in this area.
Recent data suggest that patients such as Alvin may benefit from CAR T-cell therapy in the second-line setting. Given the results discussed above and real-world comparisons to cohorts of patients with R/R DLBCL,55,56 3 RCTs compared CAR T therapy in the second-line setting to the standard of care (SOC) strategy of salvage chemoimmunotherapy and ASCT for patients with chemosensitive disease: ZUMA-7 (axi-cel), Belinda (tisa-cel), and TRANSFORM (liso-cel).57-59 All trials enrolled patients with large B-cell lymphoma who relapsed within 12 months from completion of or refractory to first-line therapy and were considered candidates for ASCT by the treating physician.
In ZUMA-7, 180 patients were randomized to receive axi-cel and 179 to receive SOC.58 The ORR and CR rate were significantly greater in the axi-cel group (83% and 65%) compared with the SOC group (50% and 32%). At a median follow-up of 24.9 months, the median EFS was 8.3 months for patients who received axi-cel and 2.0 months for patients who received SOC, and the 24-month EFS was 41% and 16%, respectively. Estimated OS at 2 years was 61% in the axi-cel group and 52% for SOC. Grade 3 or higher adverse events occurred in 91% of the patients who received axi-cel and in 83% of those who received SOC. In the TRANSFORM trial, 92 patients were randomized to receive liso-cel and 92 patients to receive SOC.59 The median EFS was 10.1 months for liso-cel vs 2.3 for SOC (HR, 0.349; P < .0001), the median PFS was 14.8 months and 5.7 months, and the CR rate was 66% and 39%, respectively. In the group receiving liso-cel, CRS grade 1 occurred in 37%, grade 2 in 11%, and grade 3 in 1 patient. Unlike the other 2 trials, the Belinda study found that CAR T-cell therapy was not superior to SOC salvage therapy.57 Patients were randomly assigned to receive tisa-cel with optional bridging therapy or salvage chemotherapy and ASCT as SOC. Approximately 26% of the patients in the tisa-cel group experienced progression at week 6, compared with approximately 14% of the patients who received SOC. Nearly 96% of the patients in the tisa-cel group received tisa-cel, and 32.5% of the patients in the SOC group received ASCT. Response occurred for 46.3% of patients receiving tisa-cel vs 42.5% of patients receiving SOC. The median EFS was 3.0 months in both groups.
Some differences in trial design that may explain these results include that Belinda allowed for multiple cycles of bridging therapy, including switching bridging therapy, whereas TRANSFORM allowed for only 1 cycle of bridging, and ZUMA-7 allowed for stabilization with steroids but no bridging therapy. In Belinda bridging chemotherapy was administered to 83% of the patients receiving tisa-cel; 48% received more than 1 cycle, and 12% received more than 1 regimen. Patients enrolled in TRANSFORM and Belinda underwent leukapheresis before randomization and were allowed to cross over from SOC. No crossover was planned in ZUMA-7, but patients were permitted to access approved CAR T-cell therapies outside the protocol. As a statistical nuance, in the assessment of EFS Belinda did not count the initiation of a second salvage or bridging regimen as an event if it occurred within the first 12 weeks. Notably, all 3 trials demonstrated very poor outcomes for patients with early R/R LBCL who underwent SOC salvage therapy and ASCT. A vibrant, detailed, and timely discussion of these trials and their implications for management of patients with early relapsed LBCL was recently presented in Blood by Drs Sehn and Westin.3 They also provide a useful algorithm for second-line therapy decision-making for DLBCL.
Patients ineligible for ASCT or CAR T therapy or who relapse after ASCT and CAR T therapy
While ASCT and CAR T have demonstrated durable remissions for patients who respond to treatment, patients who are ineligible, unable to access these therapies, or who fail treatment often experience poor outcomes. DLBCL patients in these circumstances have multiple options from recently approved therapies, including loncastuximab tesirine, polatuzumab vedotin, selinexor, and tafasitamab. However, limited data exist regarding outcomes following CAR T therapy. Loncastuximab tesirine is a CD19-directed antibody-drug conjugate that was evaluated in an international, multicenter phase 2 trial (LOTIS-2) in patients with R/R DLBCL following 2 or more lines of therapy. Among 145 patients who received at least 1 dose of loncastuximab, the ORR was 48.3% (95% CI, 39.9-56.7), including 35 patients (24%) who experienced a CR.60 The most common grade 3 or higher adverse events were neutropenia in 26%, thrombocytopenia in 18%, and increased γ-glutamyltransferase in 17%. A matching- adjusted indirect comparison was performed to evaluate the efficacy of loncastuximab compared with chemoimmunotherapy in R/R DLBCL.61 In this analysis, 80 patients from LOTIS-2 were matched by characteristics to 278 patients from pooled extension studies from CORAL, demonstrating an ORR of 53.4% in the loncastuximab cohort compared with 40.3% for chemoimmunotherapy. As exemplified below, real-world evidence comparisons are becoming more common in settings like R/R DLBCL where randomized studies are uncommon. A detailed discussion of these analyses is beyond the scope of this text, but they merit additional consideration.
The antibody-drug conjugate polatuzumab vedotin targets CD79b, a component of the B-cell receptor that is expressed on 95% of DLBCLs. Patients with R/R DLBCL ineligible for ASCT (n = 80) were randomized to receive polatuzumab vedotin combined with bendamustine and rituximab (pola-BR) or bendamustine and rituximab (BR).62 Patients who received pola-BR had a significantly higher independent review committee–assessed CR rate (40.0% vs 17.5%; P = .026), PFS (median, 9.5 vs 3.7 months; P < .001), and OS (median, 12.4 vs 4.7 months), with a median follow- up of 22.3 months. Pola-BR was associated with higher rates of grade 3 to 4 neutropenia (46.2% vs 33.3%), anemia (28.2% vs 17.9%), and thrombocytopenia (41% vs 23.1%). In a follow-up single-arm extension cohort, 106 additional patients received pola-BR, demonstrating an objective response rate of 41.5% and a CR rate of 38.7%.63 Median PFS and OS were 6.6 months and 12.5 months, respectively. No new safety signals with pola-BR were identified, and differences between the randomized arms persisted with additional follow-up. A biomarker analysis led by Dr Herrera ran a ctDNA assay based on a customized panel of recurrently mutated genes in DLBCL at baseline and end of treatment.64 Higher baseline ctDNA levels were associated with poor prognostic factors and were an independent predictor of shorter PFS, suggesting that ctDNA may be a tool for identifying patients at higher risk of progression.
Selinexor is an oral selective inhibitor of nuclear export that works by binding to exportin 1. An international multicenter phase 2 trial (SADAL) evaluated selinexor given on days 1 and 3 weekly until disease progression or unacceptable toxicity. Among 127 patients who received selinexor at 60 mg and were included in analyses of primary outcome and safety, the ORR was 28%, and the CR rate was 12%.65 The most common grade 3 to 4 adverse events were thrombocytopenia (46%), neutropenia (24%), anemia (n = 22%), and fatigue (n = 11%). Additional analyses have been performed for biological and prior-treatment subgroups.52,66
Tafasitamab is a humanized, anti-CD19 monoclonal antibody. In the international multicenter phase 2 trial L-MIND, patients with R/R DLBCL ineligible for ASCT received tafasitamab and lenalidomide for up to 12 cycles followed by tafasitamab monotherapy (in patients with stable disease or better) until disease progression.67,68 Among 80 patients who received tafasitamab plus lenalidomide, 60% (95% CI, 48%-71%) had an objective response and 43% (95% CI, 32%-54%) experienced CR. Therapy was generally well tolerated, and the most common grade 3 or higher adverse events were neutropenia (48%), thrombocytopenia (17%), and febrile neutropenia (12%). The most common nonhematological adverse effects were rash, diarrhea, asthenia, cough, peripheral edema, and fever. Tafasitamab and lenalidomide was more effective as a second-line treatment than as treatment at third line or beyond (median PFS, 23.5 months vs 7.6 months).68 In addition, it is important to note that patients with double- or triple-hit lymphoma (MYC and BCL2 and/or BCL6 rearrangement) or primary refractory disease were excluded from this study.
In a follow-up study, the median PFS was 11.6 months, and the median OS was 33.5 months.68 A retrospective observational study (RE-MIND) was performed aligning key eligibility criteria with L-MIND using data from 490 patients with R/R DLBCL who received lenalidomide monotherapy; 140 qualified for matching with the L-MIND cohort, and the primary analysis included 76 patients from each cohort.69 The analysis demonstrated significantly higher overall response from the matched group from L-MIND. A second study performed matching- adjusted indirect comparisons using data from L-MIND to match with described clinical trial cohorts such as pola-BR and gemcitabine-oxaliplatin-rituximab.70 Such approaches may increasingly be used to inform therapeutic decisions as more robust data on treatments and outcomes become available for patients with R/R DLBCL. For patients undergoing CAR T-cell therapy prior to this regimen or considering future CAR T-cell therapy following tafasitamab, it remains unclear to what extent anti-CD19 therapy or other treatments might impair the efficacy of future CD19-targeting therapies.
Clinical trials involving bispecific antibodies
Bispecific antibodies binding with 2 different cell surface antigens can direct cytotoxic T cells and other immune effector cells to areas in proximity of lymphoma cells. Several bispecific antibodies binding CD3 and CD20 are in development for DLBCL, including mosunetuzumab, glofitamab, epcoritamab, plamotamab, and odronextamab, but have some differences in structure, route of administration, and treatment schedule.71-75 Across agents, common adverse events include neutropenia, thrombocytopenia, CRS, hypophosphatemia, fatigue, and diarrhea. CRS neurological adverse events were mostly low grade and confined to cycle 1. Among 129 patients with R/R aggressive B-cell lymphoma (including 82 patients with DLBCL) treated with mosunetuzumab, the ORR was 34.9%, and the CR rate was 19.4%, with a median duration of response for all responders and complete responders of 7.6 months and 22.8 months, respectively.71 Among 19 patients who had previously undergone CAR T-cell therapy, the ORR and CR rate were 36.8% and 26.3%, respectively, but the duration of response could not be estimated due to the small sample size. In a study of 107 patients who received glofitamab, most patients were refractory to a prior CD20 antibody–containing regimen (85%), many were refractory to their initial therapy (59%), and 32% had prior CAR T. The ORR was 50%, and CR rates were 32% and 37%, respectively, among patients with and without prior CAR T.76 Epcoritamab, a subcutaneously administered CD3xCD20 bispecific antibody,73 odronextamab (REGN1979), a fully humanized bispecific immunoglobulin G4 antibody with a 14-day half-life,74 and plamotamab (XmAb13676) also have been examined in early-phase clinical trials, demonstrating meaningful ORRs and relatively similar adverse event profiles.75 For instance, a study of 157 patients who received epcoritamab demonstrated ORRs of 69% for CAR T–naive patients and 54% for patients who received prior CAR T.77 Future studies are needed to clarify the role and sequencing of bispecific antibodies relative to the current therapies available for R/R DLBCL.
Goals-of-care discussions for patients with DLBCL
Although the advent of new therapies for DLBCL has improved survival outcomes, up to 40% of patients develop R/R disease.2,3 This emphasizes that DLBCL is still a life-threatening illness, and it is thus essential for clinicians to engage in serious illness conversations with their patients. Goals-of-care discussions entail eliciting patients' goals, values, and preferences regarding their overall care as well as end-of-life (EOL) options. Ideally, these discussions should occur early and often in the DLBCL disease trajectory and should not be merely limited to EOL time points.78 Patients who have the opportunity to engage in goals-of-care discussions with their physicians are significantly more likely to receive care that is aligned with their preferences and experience higher-quality EOL care.79,80 Hematologic oncologists have an important role in initiating these conversations with patients given the trust built through longitudinal patient-physician relationships. In a retrospective study of 383 patients with hematologic malignancies, of which 37% had lymphoma, patients who had their first goals-of-care discussion with a hematologic oncologist (vs other clinicians) were significantly more likely to enroll in hospice more than 3 days before death and had lower odds of admission to the intensive care unit in the last month of life or death in the hospital.81 Such EOL outcomes are associated with a better quality of life for patients and their families, as well as a lower risk of complicated grief for bereaved caregivers.82
Goals-of-care discussions are critical and beneficial for patients with DLBCL, yet these discussions often occur too late or not at all. In a study of patients with aggressive lymphoma relapsed after first- or second-line treatment, while 44.4% had thought of their care preferences in the event of becoming critically ill, only a quarter of these patients had discussed these preferences with their clinician.83 Most hematologic oncologists (56%) in a national survey reported that goals-of-care discussions typically occur “too late,”84 and the median time between the first documented goals-of-care discussion and death was only 15 days in a study of patients who died of DLBCL or other blood cancers.81 Several barriers contribute to the current state of goals-of-care discussions. Given recent treatment advances and the potential for cure in R/R settings, the high prognostic uncertainty in DLBCL may lead some clinicians to delay discussions until death is very clearly imminent. Concerns about taking away patients' hope also contribute to hesitancy in conducting these discussions despite data showing that these conversations do not preclude hope.85 Even when clinicians grasp the importance of engaging in goals-of-care discussions, about 40% report that they do not know the right thing to say, which may result in low-quality discussions.86 Taken together, these data suggest an urgent need for strategies to improve goals-of-care discussions for DLBCL patients.
To improve timeliness of goals-of-care discussions for patients with DLBCL, it is important to start discussions before decisions are needed to avoid “crisis” communication when patients are very close to death. Having broad conversations to understand patients' values and goals for their overall care and quality of life during first-line therapy helps to set the foundation for future discussions. Practical triggers to initiate or revisit more specific goals-of-care discussions include the presence of refractory or relapsed disease (Table 2). These disease points were identified in a focus group of lymphoma clinicians as critical signposts for goals-of-care discussions.87 Other triggers identified by lymphoma clinicians include organ insufficiency or declining performance status, even in the absence of lymphoma relapse. Consideration of intensive therapies such as ASCT or CAR T-cell therapy should also prompt goals-of-care discussions. Answering no to the question “Would you be surprised if this patient died in the next year?” is also an effective trigger for engaging in these discussions.88 This question was demonstrated to correctly estimate death within 12 months in 68.3% of patients with hematologic malignancies.89 Goals-of-care discussions should not be considered one-time conversations because patients' preferences may change as their disease evolves.
Communication skills training to conduct nuanced discussions that effectively balance the potential promise of disease-directed treatments with their risks and limitations are necessary to optimize goals-of-care discussions. Tools such as the serious illness conversation guide and REMAP (reframe, expect emotion, map out patient values, align with values, and propose a plan) framework (Table 3) can help clinicians incorporate key elements of goals-of-care discussions when engaging in these conversations with DLBCL patients.77,88,90 In using these tools, clinicians should assess how much the patient understands and desires to know about the disease trajectory and prognosis and then compassionately share information tailored to the patient's preferences. It is also essential to engage the patient's loved ones in these conversations to promote alignment of goals across the family unit. These discussions should be documented in the medical record to ensure that patients' preferences are honored during care transitions. Goals-of-care skills–based training, such as VitalTalk and the Serious Illness Care Program, have effectively incorporated these communication tools.91,92 In a cluster randomized trial of the Serious Illness Care Program (a serious illness conversation guide combined with 2.5 hours of skills-based training) among 278 patients with advanced cancer, the program resulted in more frequent, earlier, and higher-quality goals-of-care discussions.93 Moreover, this intervention was associated with significant reductions in depression and anxiety symptoms.92 These findings illustrate the potential impact of optimizing goals-of-care discussions throughout the DLBCL disease course. Clinicians can apply this skill set to the discussions and care plans for each of our example patients.
Conflict-of-interest disclosure
Christopher R. Flowers: consultancy: AstraZeneca, Bayer, BeiGene, BioAscend, Bristol Myers Squibb, Celgene, Curio Sciences, Denovo Biopharma, Epizyme/Incyte, Foresight Diagnostics, Genentech/Roche, Genmab, MEI Pharmaceuticals, MorphoSys AG, Pharmacyclics/Janssen, SeaGen; stock options: Foresight Diagnostics, N Power; research funding: 4D, Abbvie, Acerta, Adaptimmune, Allogene, Amgen, Bayer, Celgene, Cellectis, EMD, Gilead, Genentech/Roche, Guardant, Iovance, Janssen Pharmaceutical, Kite, Morphosys, Nektar, Novartis, Pfizer, Pharmacyclics, Sanofi, Takeda, TGTherapeutics, Xencor, Ziopharm, Burroughs Wellcome Fund, Eastern Cooperative Oncology Group, National Cancer Institute, V Foundation, Cancer Prevention and Research Institute of Texas CPRIT Scholar in Cancer Research.
Oreofe O. Odejide: no competing financial interests to declare.
Off-label drug use
The bispecific antibodies mentioned in this article, mosunetuzumab, glofitamab, epcoritamab, plamotamab, and odronextamab, are not approved agents and their use was discussed within the context of completed and ongoing clinical trials.