

Introduction
Hemophilia is an X-linked hereditary disorder. The worldwide incidence is 1 in 5000 (hemophilia A) and 1 in 30 000 (hemophilia B).1 Treatment for hemophilia includes deficient factor replacement with clotting factor concentrates (CFCs). CFCs are also used for acute hemophilic arthritis, along with rest, ice, compression, and elevation.
There are many challenges for people with hemophilia, the most common of which are joint bleeds and deformity, which affect quality of life. Life-threatening visceral bleeding is not uncommon in hemophiliacs. Surgical intervention for hemophilia-related events that require it is always a demanding task, and the high cost of therapy is an obstacle to getting the necessary treatment. The following challenges are unique to the Indian population1-3 :
India has the second largest population of any country in the world.
India has a high patient load: the total number of registered people with hemophilia is 18 353.
Treatment for hemophilia is unaffordable for many. Less than 20% of the country’s population is covered by health insurance.
India has a diverse geography.
Many facilities that diagnose hemophilia are of poor quality.
Care is suboptimal because many treatment facilities are of poor quality.
Indians with hemophilia have a high rate of complications and disabilities.
Objective
Our aim is to study disease indications, the factors used for treatment, and the outcome of patients treated with CFCs. A subgroup analysis of patients with hemophilia A and hemophilia B was performed.
Methodology
This study used a retrospective, single-institution design. The study period was from April 1, 2017, to March 31, 2018. Included in the study were any patients with hemophilia A or B who received CFCs from the Postgraduate Institute of Medical Education and Research (PGIMER) Chandigarh.
Capacity building
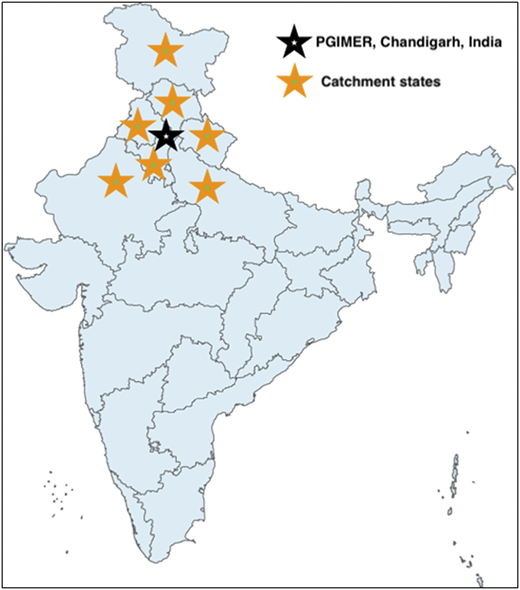
PGIMER Chandigarh is a government-run premier medical institute in northern India (Figure 1). The Hemophilia Federation India (HFI) is a nonprofit organization that has worked closely with the World Federation of Hemophilia (WFH) since 1983. HFI has worked to increase diagnosis, awareness, and affordable treatment for those with hemophilia. HFI in collaboration with WFH provides free CFCs to Indians with hemophilia. PGIMER has been associated with HFI since the 1990s. In the last year, a total of 100 patients with hemophilia received CFCs at PGIMER through this collaboration. A special CFC storage facility kept at 4°C was established to maintain factor potency (Figure 2). The free CFCs are administered by trained staff on-demand (Figure 3) to hemophilia patients who cannot afford to pay for the treatment. The collaboration is ongoing and is expected to have a profound effect on the lives of people with hemophilia.
CFCs are kept at 4°C in a storage facility established through collaborative efforts.
CFCs are kept at 4°C in a storage facility established through collaborative efforts.

A patient with hemophilia receiving intravenous factor VIII from trained staff at PGIMER Chandigarh.
A patient with hemophilia receiving intravenous factor VIII from trained staff at PGIMER Chandigarh.
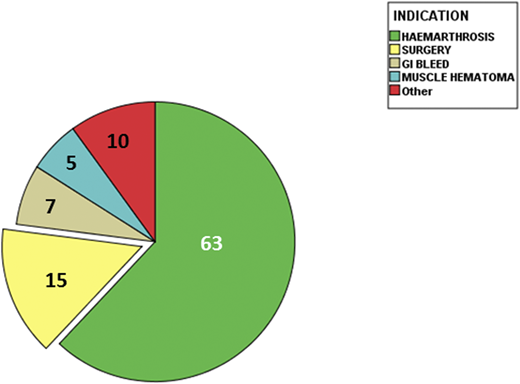
Clinical profile of patients with hemophilia who have been treated with free CFCs.
Clinical profile of patients with hemophilia who have been treated with free CFCs.
Outcome
Demographic characteristics (Figure 4):
Median age, 21 years (range, 1-54 years)
Males, 100%
Married, 40%
Mean monthly income, US$55 (range, US$11-300)
Total amount of CFCs consumed, 829 350 units
Number of patients with hemophilia A, 97
Number of patients with hemophilia B, 3
Number of patients with hemarthrosis, 63
Number of patients who underwent the following types of surgery, 15
Abdominal, 5
Craniotomy, 5
Knee arthroplasty, 2
Patella, 1
Pulmonary lobectomy, 1
Bed sore debridement, 1
Number of patients with active bleeding, 22
Gastrointestinal bleed, 7
Intracranial bleed, 5
Hematuria, 5
Muscle hematoma, 5
Discussion
CFCs are not only life saving, they are also life changing for people with hemophilia. However, the high cost of CFCs has kept them beyond the reach of people with hemophilia who live in developing world. In the last year alone, 100 people with hemophilia benefitted from the above collaboration, and 15 patients underwent successful surgical intervention with the help of free CFCs. Total consumption of CFCs was 829 350 units. Our findings support the efficacy of CFCs and emphasize that strategies are needed to overcome the high cost of CFCs for those in developing countries. Our findings also support the feasibility of global collaboration in improving the quality of life for people with hemophilia who live in developing countries.
Strengths of the study:
This study is the only study in India that has examined the effect of free CFCs on the quality of life of people with hemophilia.
The study has collected real-world data.
The collaboration enabled distribution of free CFCs to all patients included in the study.
This study was monitored by an independent observer; it was not pharma driven.
Limitations of the study:
Retrospective analysis
Single-center study
Conclusion
Collaboration between PGIMER (Chandigarh, India), HFI (New Delhi, India), and WFH (Montreal, Canada) resulted in successful implementation of life-saving and limb-saving procedures in patients with hemophilia at no cost to the patients. The collaboration emphasizes the need for similar efforts in other developing countries to bring health and a better quality of life to people suffering from hemophilia.
Authorship
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: A. Jandial, Postgraduate Institute of Medical Education and Research, Chandigarh, India; e-mail: adityapgimer@gmail.com.


