

Abstract
Frontline therapy for chronic lymphocytic leukemia (CLL) has substantially advanced in the previous decade. While monotherapy with a Bruton's tyrosine kinase (BTK) inhibitor is an excellent option for many patients, combination therapies are of high clinical interest as they can induce deep responses and durable remissions, and in many cases allow discontinuation of therapy. There are several doublet therapies that are currently in clinical use. These include combinations of BTK inhibitors (ibrutinib, acalabrutinib, zanubrutinib) or BCL2 inhibitors (venetoclax) with anti-CD20 monoclonal antibodies, and combinations of BTK and BCL2 inhibitors. While BTK inhibitors with anti-CD20 monoclonal antibodies still typically require indefinite therapy, combinations involving the BCL2 inhibitor venetoclax have allowed for successful therapy discontinuation. Triplets, which combine all 3 of these paradigms, are of interest especially for patients with higher-risk disease. While triplets have been mainly studied in single-arm trials with excellent outcomes, comparative data to doublets are limited. In this article, we outline the doublet and triplet regimens that have been evaluated in CLL as well as the data from trials comparing doublets and triplets.
Learning Objectives
Compare the different doublet regimens currently being used as standard initial treatments for CLL in terms of both efficacy and safety
Explain the potential benefit of triplet regimens in CLL relative to their risks or side effects
CLINICAL CASE
A 57-year-old woman with chronic lymphocytic leukemia (CLL) diagnosed 2 years ago presents to clinic. She now requires therapy and is experiencing progressive anemia and thrombocytopenia, symptomatic lymphadenopathy, and fatigue. Risk stratification reveals unmutated status of the immunoglobulin heavy chain variable region genes (IGHV), del(11q) on fluorescence in situ hybridization (FISH), and complex karyotype on stimulated cytogenetics. When discussing therapy, she states that her primary goal is to have a fixed-duration treatment and maximize time off therapy.
Introduction
The current paradigm of frontline CLL therapy involves targeted therapies, either covalent Bruton's tyrosine kinase inhibitor (BTKi)–based therapies or BCL2 inhibitor (BCL2i)–based therapies, or in some cases combinations of the two. Covalent BTKi produce durable remissions but rarely induce undetectable measurable residual disease (uMRD) and are therefore given continuously until disease progression, either alone or combined with 6 cycles of the anti-CD20 monoclonal antibody obinutuzumab. BCL2i, of which venetoclax is currently the only approved agent, can produce deep remissions and are generally given for a fixed duration of 1 year, initially combined with 6 cycles of obinutuzumab, or in some cases combined with the BTKi ibrutinib. In this article, we discuss the current data for doublets and triplets as frontline treatment for CLL. We also discuss ongoing clinical trials that will help determine whether doublets or triplets are better, and the open questions surrounding these types of regimens.
Doublet regimens as initial therapy for CLL
Combining 2 treatments as a “doublet” therapy in CLL has taken 2 forms: the addition of an anti-CD20 antibody to a targeted agent or combination of the 2 most established classes of targeted agents (BTKi and BCL2i). The addition of a therapeutic anti-CD20 monoclonal antibody to a targeted agent is a rational approach as its addition to cytotoxic chemotherapy as chemoimmunotherapy (CIT) improved efficacy.1,2 The combination of BTKi and BCL2i is a newer approach that has resulted in deep and durable remissions with a limited treatment duration.3,4 Here we discuss doublet regimens in practice and in trials. Doublet regimens currently used in CLL are outlined in Table 1 and Figure 1. Of note, when BTKi are combined with anti-CD20 antibodies, the BTKi is continued indefinitely, whereas when BTKi are combined with venetoclax, or when venetoclax is combined with anti-CD20 antibodies, the regimen is fixed duration.
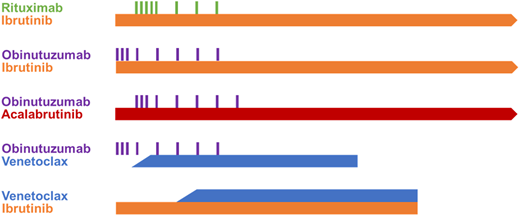
Diagram of standard doublet regimens. Standard combination treatment regimens are represented by the bars. Continuously dosed oral drugs are depicted by a solid line and infusion therapies as bars. Treatments that are continued indefinitely until disease progression or intolerable toxicity have an arrow at the right side. All treatment regimens are diagramed to scale with respect to each, with the length of the bar showing time on each drug. Ibrutinib and rituximab (IR) is based on A041202, ibrutinib and obinutuzumab (IO) on iLLUMINATE, acalabrutinib and obinutuzumab (AO) on ELEVATE-TN, venetoclax and obinutuzumab (VO) on CLL14, and venetoclax and ibrutinib on GLOW.3,6,8,10,15
Diagram of standard doublet regimens. Standard combination treatment regimens are represented by the bars. Continuously dosed oral drugs are depicted by a solid line and infusion therapies as bars. Treatments that are continued indefinitely until disease progression or intolerable toxicity have an arrow at the right side. All treatment regimens are diagramed to scale with respect to each, with the length of the bar showing time on each drug. Ibrutinib and rituximab (IR) is based on A041202, ibrutinib and obinutuzumab (IO) on iLLUMINATE, acalabrutinib and obinutuzumab (AO) on ELEVATE-TN, venetoclax and obinutuzumab (VO) on CLL14, and venetoclax and ibrutinib on GLOW.3,6,8,10,15
Phase 3 frontline studies with doublet regimens in CLL
| Agents | Study | Regimen | Patient populationa | PFS | uMRD rates | Median follow-up |
|---|---|---|---|---|---|---|
| BTKi & anti-CD20 antibody | A0412026,7 | IR | Median age: 71 | Estimated 4-year: 76% | Marrow: 2%b | 55 months |
| E19125,32 | IR | Mean age: 56.7 | Estimated 5-year: 78% | NR | 70 months | |
| iLLUMINATE8 | IO | Median age: 70 Median CIRS score: 4 | Estimated 30-month: 79% | Blood: 20%c Marrow: 30%c | 31.3 months | |
| ELEVATE-TN9,10,33 | AO | Median age: 70 CIRS >6: 16.8% | Estimated 6-year: 78% | NR | 74 months | |
| Venetoclax & anti-CD20 antibody | CLL1415,18 | VO | Median age: 72 Median CIRS score: 8 | Estimated 6-year: 53.1% Median: 76.2 months | Blood: 75.5%d Marrow: 56.9%d | 76.4 months |
| GIAIA/CLL1311 | VR | Median age: 62 Median CIRS score: 2 | Estimated 4-year: 70.1% | Blood: 57.0%e Marrow: 43.0%f | 50.7 months | |
| GIAIA/CLL1311 | VO | Median age: 62 Median CIRS score: 2 | Estimated 4-year: 81.8% | Blood: 85.6%e Marrow: 72.5f | 50.7 months | |
| BTKi & venetoclax | GLOW3 | IV | Median age: 71 Median CIRS score: 9 | Estimated 2-year: 84.4% | Blood: 54.7%d Marrow: 51.9%d | 27.2 months |
| FLAIR24 | IV | Median age: 62 | Estimated 3-year: 97.2% | Blood: 92.7%g Marrow: 65.9%g | 43.7 months |
| Agents | Study | Regimen | Patient populationa | PFS | uMRD rates | Median follow-up |
|---|---|---|---|---|---|---|
| BTKi & anti-CD20 antibody | A0412026,7 | IR | Median age: 71 | Estimated 4-year: 76% | Marrow: 2%b | 55 months |
| E19125,32 | IR | Mean age: 56.7 | Estimated 5-year: 78% | NR | 70 months | |
| iLLUMINATE8 | IO | Median age: 70 Median CIRS score: 4 | Estimated 30-month: 79% | Blood: 20%c Marrow: 30%c | 31.3 months | |
| ELEVATE-TN9,10,33 | AO | Median age: 70 CIRS >6: 16.8% | Estimated 6-year: 78% | NR | 74 months | |
| Venetoclax & anti-CD20 antibody | CLL1415,18 | VO | Median age: 72 Median CIRS score: 8 | Estimated 6-year: 53.1% Median: 76.2 months | Blood: 75.5%d Marrow: 56.9%d | 76.4 months |
| GIAIA/CLL1311 | VR | Median age: 62 Median CIRS score: 2 | Estimated 4-year: 70.1% | Blood: 57.0%e Marrow: 43.0%f | 50.7 months | |
| GIAIA/CLL1311 | VO | Median age: 62 Median CIRS score: 2 | Estimated 4-year: 81.8% | Blood: 85.6%e Marrow: 72.5f | 50.7 months | |
| BTKi & venetoclax | GLOW3 | IV | Median age: 71 Median CIRS score: 9 | Estimated 2-year: 84.4% | Blood: 54.7%d Marrow: 51.9%d | 27.2 months |
| FLAIR24 | IV | Median age: 62 | Estimated 3-year: 97.2% | Blood: 92.7%g Marrow: 65.9%g | 43.7 months |
aAge reported in years. bAfter 8 cycles of treatment. cCollected prior to subsequent treatment. dAssessed 3 months after treatment completion. eAt month 15 of treatment. fAt final restaging in patients with a compete remission. gAt 5 years of treatment.
Regimens: AO, acalabrutinib and obinutuzumab; BTKi, BTK inhibitor; IO, ibrutinib and obinutuzumab; IR, ibrutinib and rituximab; IV, ibrutinib and venetoclax; VO, venetoclax and obinutuzumab; VR, venetoclax and rituximab. CIRS, Cumulative Illness Rating Scale; NR, not reported; PFS, progression-free survival; uMRD, undetectable measurable residual disease.
Covalent BTK inhibitors and anti-CD20 antibodies
Doublets of a BTKi with an anti-CD20 monoclonal antibody include 3 FDA-approved combinations: ibrutinib plus rituximab (IR), ibrutinib plus obinutuzumab (IO), and acalabrutinib plus obinutuzumab (AO).
IR was compared with fludarabine, cyclophosphamide, and rituximab (FCR) in a study of young (<70 years) fit patients without del(17p) undergoing initial treatment in E1912. There was a benefit in both PFS and OS with IR over FCR.5 However, the A041202 trial demonstrated no improvement in PFS for IR compared with ibrutinib alone in older patients with treatment-naïve CLL, with an estimated 48-month PFS of 76% for both groups, suggesting that for most patients, single-agent ibrutinib is preferred over IR.6,7 In the iLLUMINATE study, where ibrutinib was combined with obinutuzumab and 42-month PFS was 74%, patients with IGHV-mutated disease had significantly longer PFS, but there was no difference based on the presence of TP53 abnormalities.8 Based on these studies, both IR and IO are FDA-approved regimens for frontline CLL.
In contrast, the ELEVATE-TN study, which compared acalabrutinib with AO, demonstrated improved PFS advantage to AO over acalabrutinib, although in a post hoc exploratory analysis.9 Here, the estimated 72-month PFS was 62% and 78% for acalabrutinib and AO, respectively.9 The PFS benefit with the addition of obinutuzumab did not appear to extend to patients with del(17p). The benefit of AO must be weighed against the risk of extra toxicity, especially of infusion reactions and neutropenia.10
The differences between IR and AO could be due to the antibody as obinutuzumab has been demonstrated to be more effective than rituximab in combinations with other drugs.11,12 The BTKi used may also be important as in ex vivo studies, antibody-dependent cellular phagocytosis was less inhibited with acalabrutinib compared with ibrutinib.13 The third approved covalent BTKi, zanubrutinib, has been studied in combination with obinutuzumab in a phase 1 study that found the combination to be safe and tolerable, but efficacy data are not definitive.14
Venetoclax and anti-CD20 antibodies
BCL2 inhibition has been an important addition to our current therapies for CLL. While there are several BCL2i in clinical development, most of the available data are for venetoclax. Treatment regimens that combined venetoclax with an anti-CD20 antibody for a fixed-duration treatment were developed and entered phase 3 testing without large studies of venetoclax continuous monotherapy; therefore, data to help us understand the additive benefit of the anti-CD20 monoclonal antibody are limited.15,16 The strength of these combinations is that they allow venetoclax to be fixed-duration due to high rates of uMRD.
The standard initial treatment regimen of venetoclax and obinutuzumab (VO) was compared with CIT with O-Clb in patients with comorbidities in the CLL14 study and also compared in a 4-arm trial with CIT, venetoclax and rituximab (VR), and ibrutinib, venetoclax, and obinutuzumab (IVO) in the GAIA/CLL13 study, which included fit patients and excluded del(17p) CLL.11,15 In both studies venetoclax was given for 12 cycles of 28 days with obinutuzumab given for the first 6 cycles, and responses off treatment were quite durable. The median PFS for VO in the CLL14 study was 76.2 months with a median follow-up of 76.4 months, and the estimated 5-year PFS was 62.6%.17,18 The PFS was longer in patients with IGHV-mutated CLL, making this an even better choice for patients in this group.17 While there was shorter follow-up with the GAIA/CLL13 study, the results were also favorable, demonstrating improved PFS with VO compared with CIT, with a median follow-up of 50.7 months.19 Notably, although the trial was not powered for this comparison, the PFS for VO was also better than VR (hazard ratio 0.57, p0.0011), suggesting that obinutuzumab is the most appropriate antibody to add to venetoclax in this setting.
The evidence supports VO in both fit patients and those with comorbidities. As well, while patients with high-risk genomic features (TP53 abnormalities or IGHV unmutated status) have shorter remission than those with standard-risk disease, high-risk patients do significantly better with VO than with CIT, making VO an appropriate option for these patients.20
BTK inhibitors and venetoclax
The approach of an ibrutinib and venetoclax (IV) doublet was well studied in phase 2 trials. The approach was first reported in a phase 2 study that included 24 cycles of IV. This study proved that the approach was safe and feasible, with high rates of bone marrow uMRD.21 The larger phase 2 CAPTIVATE study enrolled fit patients ≤70 years of age who were receiving initial treatment for CLL. There were 2 cohorts: a fixed-duration cohort in which everyone stopped treatment after 15 total cycles and an MRD cohort in which patients were randomized to receive additional treatment depending on their MRD status.4,22 Results pooled from the FD cohort and the placebo arm of the MRD cohort who were treated similarly were reported at a median follow-up of 56 months, and the estimated 54-month PFS was 70%.23 Importantly, no mutations conferring resistance to venetoclax or ibrutinib were detected in patients at the time of relapse. As the CAPTIVATE study enrolled younger fit patients, it is generally used to support use of IV in this group.
There are 2 phase 3 trials comparing IV with CIT. The GLOW study enrolled patients who were older (≥65 years) or who had comorbidities and compared IV with O-Clb.3 Results demonstrated improved PFS with IV, with a 24-month PFS of 84.4%. This study led to the approval of IV as a standard regimen by European agencies but not in the United States. However, the National Comprehensive Cancer Network Guidelines support consideration for this as a standard regimen in the United States, despite lack of FDA approval.
The FLAIR trial took a different approach. FLAIR randomized fit patients without del(17p) CLL to either FCR or IV with an MRD-guided discontinuation approach that allowed for up to 6 years of treatment.24 The estimated 3-year PFS was 97.2% for IV compared with 76.8% with FCR; however, therapy duration was extended in many cases, with only 56% of patients stopping IV before 60 months. The shorter fixed-duration regimen approved in Europe based on the GLOW trial spares patients the toxicity of extended treatment and is more commonly used than the MRD-guided approaches at this time.
Zanubrutinib plus venetoclax (ZV) has also been studied in treatment-naïve CLL with TP53 abnormalities as an arm of the SEQUOIA study. Here, ZV was administered for 24 cycles after a 3-cycle lead-in of zanubrutinib, and then zanubrutinib monotherapy was continued until disease progression. uMRD was achieved in the blood in 48% of patients, with a 3-year PFS of 92%.25
Triplet regimens as initial therapy for CLL
Novel therapy triplet combinations that have been evaluated in CLL are those that include a BTKi, a BCL2i, and an anti-CD20 antibody. Thus far, all the data are for a covalent BTKi, venetoclax, and obinutuzumab; however, ongoing studies are evaluating noncovalent BTKi and other BCL2i. Triplet regimens likely add toxicity over doublet approaches, and no presented or published data have yet compared a triplet with a BTKi/BCL2i doublet regimen. Despite this, there is interest in triplet regimens, especially for patients with higher-risk disease. Currently, triplets are generally used only in clinical trials, and no triplets have been approved by regulatory agencies or recommended by the National Comprehensive Cancer Network for use. Triplet regimens are outlined in Table 2 and Figure 2.
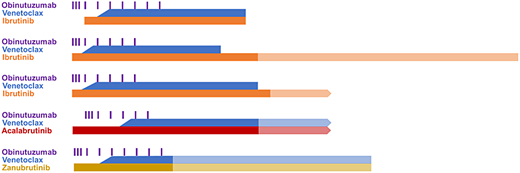
Diagram of triplet regimens. Triplet treatment regimens are represented by the bars. Continuously dosed oral drugs are depicted by a solid line and infusion therapies as bars. Regimens that used an MRD or response-guided approach to determine if treatment was discontinued have a translucent bar to indicate that some patients continued treatment. Treatments that are continued indefinitely with no set timepoint to end have an arrow at the right side. All treatment regimens are diagramed to scale with respect to each, with the length of the bar showing time on each drug. The ibrutinib, venetoclax, and obinutuzumab (IVO) diagrams are based on multiple studies: a phase 2 study; the CLL2-GIVe and GAIA/CLL13 studies, which used the same treatment; and AO41702.19,26,28 The AVO and ZVO diagrams are based on the phase 2 studies with these regimens.29,30
Diagram of triplet regimens. Triplet treatment regimens are represented by the bars. Continuously dosed oral drugs are depicted by a solid line and infusion therapies as bars. Regimens that used an MRD or response-guided approach to determine if treatment was discontinued have a translucent bar to indicate that some patients continued treatment. Treatments that are continued indefinitely with no set timepoint to end have an arrow at the right side. All treatment regimens are diagramed to scale with respect to each, with the length of the bar showing time on each drug. The ibrutinib, venetoclax, and obinutuzumab (IVO) diagrams are based on multiple studies: a phase 2 study; the CLL2-GIVe and GAIA/CLL13 studies, which used the same treatment; and AO41702.19,26,28 The AVO and ZVO diagrams are based on the phase 2 studies with these regimens.29,30
Reported frontline studies with triplet regimens in CLL
| Agents | Study | Regimen | Patient population | PFS | uMRD rate | Median follow-up |
|---|---|---|---|---|---|---|
| Ibrutinib-venetoclax-obinutuzumab | Phase 2 | IVO | Median age: 58 | Median: 88.5 months | Marrow: 56%a | 85.6 months (first 25 TN patients) |
| CLL2-GIVe | IVO | Median age: 62 All patients had altered TP53 | Estimated 3-year: 79.9% | Blood: 78%b | NR | |
| GAIA/CLL1319 | IVO | Mean age: 60.7 Median CIRS score: 2 | Estimated 4-year: 85.5% | Blood: 92.2%c | 50.7 months | |
| A04170228 | IVO | Median age: 74 | Estimated 18-month: 85% | Marrow: 86.7%d | 14 months | |
| Acalabrutinib-venetoclax-obinutuzumab | Phase 229 | AVO | Median age: 63 | At 27.6 months: 100% | Blood: 86%e Marrow: 86% | 27.6 months |
| Zanubrutinib-venetoclax-obinutuzumab | BOVen30 | ZVO | Median age: 62 | One progression event, 2 deaths | Both blood and marrow: 89%f | 25.8 months |
| Agents | Study | Regimen | Patient population | PFS | uMRD rate | Median follow-up |
|---|---|---|---|---|---|---|
| Ibrutinib-venetoclax-obinutuzumab | Phase 2 | IVO | Median age: 58 | Median: 88.5 months | Marrow: 56%a | 85.6 months (first 25 TN patients) |
| CLL2-GIVe | IVO | Median age: 62 All patients had altered TP53 | Estimated 3-year: 79.9% | Blood: 78%b | NR | |
| GAIA/CLL1319 | IVO | Mean age: 60.7 Median CIRS score: 2 | Estimated 4-year: 85.5% | Blood: 92.2%c | 50.7 months | |
| A04170228 | IVO | Median age: 74 | Estimated 18-month: 85% | Marrow: 86.7%d | 14 months | |
| Acalabrutinib-venetoclax-obinutuzumab | Phase 229 | AVO | Median age: 63 | At 27.6 months: 100% | Blood: 86%e Marrow: 86% | 27.6 months |
| Zanubrutinib-venetoclax-obinutuzumab | BOVen30 | ZVO | Median age: 62 | One progression event, 2 deaths | Both blood and marrow: 89%f | 25.8 months |
aAt end of therapy; bAt cycle 12; cAt month 15; dAt cycle 15; eAt start of cycle 16; fBest uMRD at follow-up.
Regimens: AVO, acalabrutinib, venetoclax, and obinutuzumab; IVO, ibrutinib, venetoclax, and obinutuzumab; ZVO, zanubrutinib, venetoclax, and obinutuzumab. NR, not reported; PFS, progression-free survival; uMRD, undetectable measurable residual disease.
Estimated 4-year: 85.5%.
Ibrutinib-based triplets
IVO triplets have been the most frequent triplets studied in CLL. Initial data come from a phase 1/2 study, where 50 patients with treatment-naïve CLL were enrolled in 2 time-disparate cohorts. uMRD was achieved in the bone marrow of 58% of patients.26 For the 25 patients with long-term follow-up, median PFS was 88.5 months. The phase 2 CLL2-GIVe study also evaluated this combination in 41 patients with high-risk CLL with TP53 alterations.27 In this study, ibrutinib could be continued until cycle 13 in patients who had not achieved a uMRD complete response (CR). At cycle 15, the CR rate was 58.5%, and peripheral blood uMRD was 78%. The 36-month PFS was 79.9%.27
IVO has also been evaluated in 2 phase 3 trials. The GAIA/CLL13 study included a cohort of patients treated with IVO.19 Ibrutinib could be continued up to 36 cycles or until MRD was undetectable. The peripheral blood uMRD rate in the IVO arm at month 15 was 92.2%, and 4-year PFS was 85.5%. IVO was declared superior to chemoimmunotherapy (CIT) in this study (hazard ratio 0.30, p < 0.001). The PFS from the IVO arm looks similar to the PFS from the VO arm, but long-term follow-up will be of high interest.19
The phase 3 A041702 also evaluated IVO, here compared with IO in patients ≥65 years. IVO could be discontinued after 14 cycles in patients with a uMRD CR, and others continued ibrutinib indefinitely.28 Bone marrow uMRD was 86.6% in the IVO arm after 14 cycles, and CR rate was 68.5%. Unfortunately, this study was heavily affected by the COVID-19 pandemic, and due to a higher death rate on the IVO arm, the futility boundary was crossed. The 18-month PFS with IVO was 85%, however, when deaths due to COVID-19 were censored, and 18-month PFS was 94%.28 A similar phase 3 study in younger fit patients comparing IO to IVO with a fixed duration is being conducted through ECOG and has not yet been reported. The primary endpoint was noninferiority, and the impact of COVID-19 may have been less in this younger patient population. Those results are also eagerly awaited to help us determine the relative benefit of triplet therapy.
Newer BTKi-based triplets
Limited data exist for the combinations of acalabrutinib plus venetoclax plus obinutuzumab (AVO) and zanubrutinib plus venetoclax plus obinutuzumab (ZVO). AVO was investigated in a multicenter phase 2 trial. AVO was given for 15 cycles, and acalabrutinib could be stopped at the end of cycle 15 if a uMRD CR was achieved, or at the end of cycle 24 if uMRD was achieved with any response; otherwise acalabrutinib was continued indefinitely. The best rate of peripheral blood MRD was 92%, and bone marrow MRD was 86%, with all patients remaining in remission at a median follow-up of 27.6 months.29 In a cohort of this study restricted to patients with TP53-altered disease, 45% achieved a CR with uMRD in the bone marrow.
ZVO was investigated in the frontline setting in the phase 2 BOVen study.30 In this trial, triplet therapy was discontinued in an MRD-guided manner, where patients could receive between 8 and 24 cycles of therapy. Of 37 patients who underwent response evaluations, 89% achieved uMRD in the blood and bone marrow, and 57% of patients had a CR. With a median follow-up of 25.8 months, only 1 patient experienced disease progression. Treatment was also limited duration in most cases, with 89% of patients discontinuing therapy after a median of 10 cycles.30 While follow-up with both ZVO and AVO so far is short, the results of uMRD are promising.
One noncovalent BTKi, pirtobrutinib, has also been studied in combination with venetoclax and obinutuzumab (PVO). Very early data are promising, with 92% achieving uMRD at a level of 10−4 and 76% at 10−6 in bone marrow at cycle 7.31
Comparisons between doublets and triplets
A number of clinical trials have or are comparing standard doublets of BTKi plus obinutuzumab or VO to a triplet regimen. Ongoing phase 3 studies are outlined in Table 4. With ibrutinib, as mentioned, the GAIA/CLL13 study included arms of VO and IVO. With current follow-up, these 2 arms do not appear significantly different. As well, the A041702 study did not find that IVO was superior to IO; however, a similar study in younger patients, EA9161, is ongoing. With acalabrutinib, the CLL16 study is currently comparing AVO with VO in patients with TP53-altered or complex karyotype CLL. It will be highly interesting to see if differences emerge in PFS with longer follow-up or newer BTKi.
Direct comparisons between BTKi/venetoclax doublets and triplets are lacking. Tables 1 and 2 outline efficacy endpoints in respective doublet and triplet regimens. However, comparison among studies is extremely difficult, as therapy duration and patient populations are not consistent among studies. The only current trial comparing a BTKi/venetoclax doublet with a triplet is the phase 3 Amplify study (NCT03836261), which is comparing AV and AVO to chemoimmunotherapy. Given that acalabrutinib is the only BTKi that has demonstrated superiority of a BTKi plus antibody to BTKi alone, if this trial does not demonstrate an advantage to adding obinutuzumab to AV, this will likely end interest in obinutuzumab-based triplet regimens for standard-risk patients. However, there may still be interest in investigating triplets vs doublets for those at high risk of relapse after therapy completion, and this could be addressed in future studies. Longer follow-up of current studies or future ones in specific patient subtypes, such as those with del(17p), will likely be needed to determine which patients might most benefit from triplet therapies.
In addition to efficacy, safety of triplets vs doublets is of high interest. Table 3 outlines key toxicities seen with these combinations across studies. With variation in follow-up, it is difficult to discern substantive differences in toxicity, except potentially higher rates of hematologic toxicity. While acalabrutinib- and zanubrutinib-based combinations are thought to be safer than ibrutinib-based, direct comparisons are not available. Given the variety of options available for our patients today, the safety profile of any regimen and the individual patient's comorbidities should always be carefully considered.
Rate of select adverse events with select doublet and triplet regimens
| Adverse event | AO (ELEVATE TN)a | VO (CLL14)b | IV (Captivate FD cohort)c | IV (GLOW)d | IVO (GAIA/CLL13)e | AVO (phase 2)f | ZVO (BOVen)g |
|---|---|---|---|---|---|---|---|
| Grade 3+ neutropenia | 30.9% | 52.8% | 33% | 34.9% | 48% | 43% | 18% |
| Grade 3+ thrombocytopenia | NR | 14.2% | 13% | 5.7% | 16% | 27% | 8% |
| Hypertension | 7.9% | 3.3% (G3+) | 16% | 7.5% (G3+) | 12.5% | 11% | 13% |
| Atrial fibrillation | 3.9% | 2.4% (G3+) | 4% | 6.6% (G3+) | 7.8% | 3% | 2.5% |
| Grade 3+ bleeding or major bleeding | 2.8% | NR | 2% | NR | NR | 0 | 3% |
| Infection | 75.3% | NR | 67% | NR | NR | 14% | NR |
| Grade 3+ infection | 23.6% | NR | 8% | 17% | NR | 3% | NR |
| Secondary malignancies total/total minus nonmelanoma skin cancers | 15.7%/8.4% | 22.2%/13.2% | NR | 0.9% | 17% | NR | NR |
| Discontinuation of therapy for AE | 13% | 16% | 1% | 10.4% | NR | NR | NR |
| Adverse event | AO (ELEVATE TN)a | VO (CLL14)b | IV (Captivate FD cohort)c | IV (GLOW)d | IVO (GAIA/CLL13)e | AVO (phase 2)f | ZVO (BOVen)g |
|---|---|---|---|---|---|---|---|
| Grade 3+ neutropenia | 30.9% | 52.8% | 33% | 34.9% | 48% | 43% | 18% |
| Grade 3+ thrombocytopenia | NR | 14.2% | 13% | 5.7% | 16% | 27% | 8% |
| Hypertension | 7.9% | 3.3% (G3+) | 16% | 7.5% (G3+) | 12.5% | 11% | 13% |
| Atrial fibrillation | 3.9% | 2.4% (G3+) | 4% | 6.6% (G3+) | 7.8% | 3% | 2.5% |
| Grade 3+ bleeding or major bleeding | 2.8% | NR | 2% | NR | NR | 0 | 3% |
| Infection | 75.3% | NR | 67% | NR | NR | 14% | NR |
| Grade 3+ infection | 23.6% | NR | 8% | 17% | NR | 3% | NR |
| Secondary malignancies total/total minus nonmelanoma skin cancers | 15.7%/8.4% | 22.2%/13.2% | NR | 0.9% | 17% | NR | NR |
| Discontinuation of therapy for AE | 13% | 16% | 1% | 10.4% | NR | NR | NR |
aMedian follow-up 46.9 months; bMedian follow-up 66.7 months; cMedian follow-up 27.9 months; dMedian follow-up 27.7 months; eMedian follow-up 50.7 months; fMedian follow-up 27.6 months; gMedian follow-up 25.8 months.
NR, not reported.
Ongoing phase 3 trials of doublets and triplets in treatment-naive CLL
| Trial name/ID | Patient population | Therapies investigated | Other information |
|---|---|---|---|
| CELESTIAL-TNCLL NCT06073821 | Treatment-naive | Zanubrutinib plus sonrotoclax vs venetoclax plus obinutuzumab | 1-year fixed duration in both arms |
| MAJIC NCT05057494 | Treatment-naive | Acalabrutinib plus venetoclax vs venetoclax plus obinutuzumab | Both arms are MRD guided with a maximum of 2 years treatment |
| AMPLIFY NCT03836261 | Treatment-naive without del(17p) | Acalabrutinib plus venetoclax plus obinutuzumab or acalabrutinib plus venetoclax vs chemoimmunotherapy | Both acalabrutinib arms are 1-year fixed duration |
| CLL16 NCT05197192 | High-risk treatment-naive (del17p, TP53 mutated, or complex karyotype) | Acalabrutinib plus venetoclax plus obinutuzumab vs venetoclax plus obinutuzumab | Acalabrutinib for 24 cycles, venetoclax for 12 cycles in AVO arm |
| EA9161 NCT03701282 | Treatment-naive under age 70 years without del17p | Ibrutinib plus venetoclax plus obinutuzumab vs ibrutinib plus obinutuzumab | IVO is 18 months fixed duration for all patients |
| CLL17 NCT04608318 | Treatment-naive | Ibrutinib vs venetoclax plus obinutuzumab vs ibrutinib plus venetoclax | 1-year fixed duration in both venetoclax-containing arms |
| Trial name/ID | Patient population | Therapies investigated | Other information |
|---|---|---|---|
| CELESTIAL-TNCLL NCT06073821 | Treatment-naive | Zanubrutinib plus sonrotoclax vs venetoclax plus obinutuzumab | 1-year fixed duration in both arms |
| MAJIC NCT05057494 | Treatment-naive | Acalabrutinib plus venetoclax vs venetoclax plus obinutuzumab | Both arms are MRD guided with a maximum of 2 years treatment |
| AMPLIFY NCT03836261 | Treatment-naive without del(17p) | Acalabrutinib plus venetoclax plus obinutuzumab or acalabrutinib plus venetoclax vs chemoimmunotherapy | Both acalabrutinib arms are 1-year fixed duration |
| CLL16 NCT05197192 | High-risk treatment-naive (del17p, TP53 mutated, or complex karyotype) | Acalabrutinib plus venetoclax plus obinutuzumab vs venetoclax plus obinutuzumab | Acalabrutinib for 24 cycles, venetoclax for 12 cycles in AVO arm |
| EA9161 NCT03701282 | Treatment-naive under age 70 years without del17p | Ibrutinib plus venetoclax plus obinutuzumab vs ibrutinib plus obinutuzumab | IVO is 18 months fixed duration for all patients |
| CLL17 NCT04608318 | Treatment-naive | Ibrutinib vs venetoclax plus obinutuzumab vs ibrutinib plus venetoclax | 1-year fixed duration in both venetoclax-containing arms |
CLINICAL CASE (continued)
Given our patient's preference for a fixed-duration therapy, a venetoclax-containing doublet would be the best standard of care option. While her higher-risk features of unmutated IGHV and complex karyotype may result in a shorter PFS, this is still a reasonable option. Currently there are no reported studies comparing VO with IV, so the decision would be made based on her comorbidities and preferences regarding potential side effects and route of administration.
The patient was highly interested in the idea that adding an antibody to a BTKi and BCL2i combination might prolong her response. She was also enthusiastic about helping to answer this question for patients who might be in her position in the future. She therefore chose to enroll in a phase 3 study of a triplet vs doublet therapy.
Conclusions
While remarkable progress has been made in CLL, several key questions remain regarding combination therapy. These include the best drug to use in each class, considerations for individual CLL characteristics that benefit most or least from combination regimens, sequencing of therapies over the patient's lifespan, and incorporation of novel agents as they are developed. While we have not observed resistance mutations with fixed-duration combination regimens, broad experience with retreatment is lacking. Thoughtfully designed trials, including phase 3 studies, will be needed to answer these questions and best advise our patients.
Acknowledgments
K.A.R. and J.A.W. are scholars in clinical research of the Leukemia and Lymphoma Society. They acknowledge all the patients who participated in the clinical trials that made this information possible and their colleagues whose dedication to thoughtful clinical trials continues to advance the field.
Conflict-of-interest disclosure
Kerry A. Rogers receives research funding from Genentech, AbbVie, Novartis, AstraZeneca, and LOXO@Lilly and consults for Pharmacyclics, Janssen, AstraZeneca, LOXO@Lilly, BeiGene, Genentech, AbbVie, and Alpine Immune Sciences.
Jennifer A. Woyach receives research funding from AbbVie, Beigene, Janssen, Pharmacyclics, and Schrödinger and consults for AbbVie, AstraZeneca, Beigene, Genentech, LOXO@Lilly, Merck, Newave, and Pharmacyclics.
Off-label drug use
Kerry A. Rogers: Off-label drug use is only described in the context of clinical trials.
Jennifer A. Woyach: Off-label drug use is only described in the context of clinical trials.
