

Abstract
The multifaceted pathophysiologic processes that comprise thrombosis and thromboembolic diseases take on a particular urgency in the hospitalized setting. In this review, we explore 3 cases of thrombosis from the inpatient wards: purpura fulminans, cancer-associated thrombosis with thrombocytopenia, and coronavirus disease 2019 (COVID-19) and the use of dose-escalated anticoagulation therapy and antiplatelet agents. We discuss the evaluation and management of purpura fulminans and the roles of plasma transfusion, protein C and antithrombin replacement, and anticoagulation in treating this disease. We present a framework for evaluating the etiologies of thrombocytopenia in cancer and review 2 strategies for anticoagulation management in patients with cancer-associated thrombosis and thrombocytopenia, including recent prospective data supporting the use of dose-modified anticoagulation based on platelet count. Last, we dissect the major clinical trials of therapeutic- and intermediate-dose anticoagulation and antiplatelet therapy in hospitalized patients with COVID-19, reviewing key recommendations from consensus guidelines while highlighting ways in which institutional and patient-tailored practices regarding antithrombotic therapies in COVID-19 may differ. Together, the cases highlight the diverse and dramatic presentations of macro- and microvascular thrombosis as encountered on the inpatient wards.
Learning Objectives
Review the evaluation and management of purpura fulminans
Describe approaches to anticoagulation management in cancer-associated thrombosis and thrombocytopenia
Discuss the use of anticoagulation and antiplatelet therapy in COVID-19
CLINICAL CASE 1
A 37-year-old man is admitted for fever and fatigue. On initial presentation, he is in shock, requiring fluid resuscitation and vasopressor support. He is treated with broad-spectrum intravenous antibiotics. Physical examination reveals tender, retiform (ie, angulated) purpura on his trunk and bilateral extremities, erythematous bullous lesions surrounding central areas of hemorrhagic necrosis, and dusking of his fingertips and toes (Figure 1A-C). Laboratory studies show a prolonged prothrombin time (PT), prolonged activated partial thromboplastin time (aPTT), decreased fibrinogen, increased fibrin split products, and a platelet count of 45 000/µL. Blood cultures return positive for Haemophilus influenzae. A skin biopsy specimen of a necrotic skin lesion shows small vessel thrombosis with red cell extravasation (Figure 1D). The Hematology service is consulted due to concern for purpura fulminans (PF).
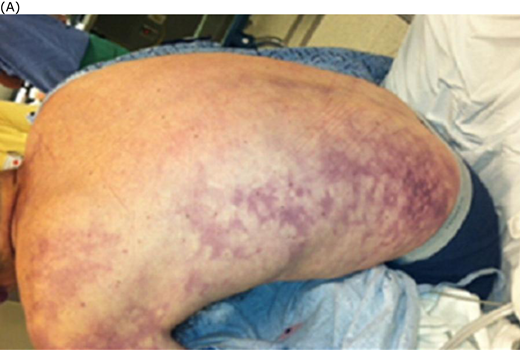


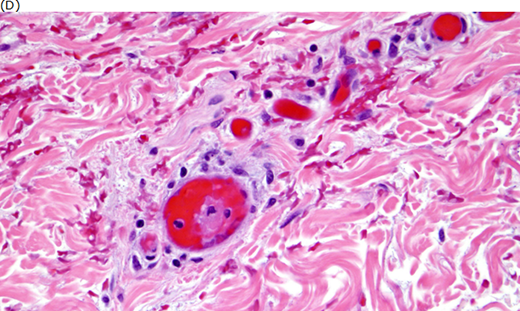
(A) Retiform purpura, (B) bullous skin necrosis, (C) peripheral dusking, and (D) microvascular thrombosis in purpura fulminans. Adapted from Colling and Bendapudi1 (A, C, and D) and from Davis MDP et al.43
Question 1: How do we evaluate and treat purpura fulminans?
Pathophysiology
Described in 1884, PF is a rare, life-threatening disorder representing an extreme thrombotic phenotype of disseminated intravascular coagulation.1 At least 3 distinct PF types have been characterized: inherited, autoimmune, or postinfectious (also termed idiopathic) and, most commonly, acute infectious (Table 1). Mechanistically, all 3 are mediated in part by reductions in the activity of endogenous anticoagulants, most notably the protein C (PC) system and antithrombin, in concert with uncontrolled tissue factor expression by leukocytes and/or endothelium stemming from the inflammatory response.
Classification of purpura fulminans
| Inherited | Autoimmune or postinfectious (“idiopathic”) | Acute infectious | |
|---|---|---|---|
| Mechanism | Inherited PC or rarely PS deficiency | Neutralizing antibodies against PS or rarely PC | Aberrant tissue factor expression with concomitant failure of thrombomodulin-PC system |
| Associations | • Varicella zoster virus • Human herpesvirus 6 | • Neisseria meningitidis • Haemophilus influenza • Streptococcus pneumoniae • Other encapsulated organisms • Staphylococcus aureus • Capnocytophaga canimorsus • Rickettsial infection • Plasmodium falciparum | |
| Clinical setting | Neonatal | Within 2 weeks after viral infection | Septic shock |
| Rash distribution | Lower half of body > upper half | Lower half of body > upper half | Distal to proximal progression (worse in acral areas) or diffuse from onset |
| Laboratory findings | • Thrombocytopenia • Elevated D-dimer or fibrin split products • Hypofibrinogenemia • Prolonged PT and/or aPTT • Low PC, PS, and antithrombin activity | ||
| Inherited | Autoimmune or postinfectious (“idiopathic”) | Acute infectious | |
|---|---|---|---|
| Mechanism | Inherited PC or rarely PS deficiency | Neutralizing antibodies against PS or rarely PC | Aberrant tissue factor expression with concomitant failure of thrombomodulin-PC system |
| Associations | • Varicella zoster virus • Human herpesvirus 6 | • Neisseria meningitidis • Haemophilus influenza • Streptococcus pneumoniae • Other encapsulated organisms • Staphylococcus aureus • Capnocytophaga canimorsus • Rickettsial infection • Plasmodium falciparum | |
| Clinical setting | Neonatal | Within 2 weeks after viral infection | Septic shock |
| Rash distribution | Lower half of body > upper half | Lower half of body > upper half | Distal to proximal progression (worse in acral areas) or diffuse from onset |
| Laboratory findings | • Thrombocytopenia • Elevated D-dimer or fibrin split products • Hypofibrinogenemia • Prolonged PT and/or aPTT • Low PC, PS, and antithrombin activity | ||
In patients with infectious PF, skin biopsy specimens typically show microvascular thrombosis without endothelial cell perturbation during the initial phases of the disease, which progresses to endotheliopathy and tissue necrosis over subsequent days, with loss of endothelial thrombomodulin and consequent failure of the thrombomodulin-PC system.2 It has recently been suggested that rare germline mutations in the complement system predispose patients to developing infectious PF by triggering a maladaptive hyperinflammatory response to infection.3 By contrast, inherited PF occurs in neonates with severe congenital deficiency of PC or, rarely, protein S (PS). Autoimmune or postinfectious PF typically occurs as a result of inhibitory autoantibodies against PS or, less commonly, PC, arising within a couple weeks after viral infection.
Clinical presentation and laboratory findings
PF is characterized by the development of erythematous macular skin lesions on the trunk and extremities; the exact distribution of lesions may vary slightly depending on etiology (Table 1). These often form a reticular pattern representing occlusion of the microvasculature. A dusky appearance of acral areas and distal extremities indicating microvascular tissue ischemia is common early in the disease. As PF progresses, the lesions develop central necrosis, with bullae in hemorrhagic areas. Acute infectious PF typically develops in the setting of septic shock; Neisseria meningitidis is the most common causative microorganism and may rarely present with adrenal hemorrhage as part of the Waterhouse- Friderichsen syndrome. Additional associated microbes include Haemophilus influenzae, Streptococcus pneumoniae, Capnocytophaga canimorsus, other encapsulated organisms, and Staphylococcus aureus. Inherited PF presents in the neonatal period, while idiopathic or postinfectious PF typically arises within 2 weeks of exposure to varicella or human herpesvirus 6.1 Laboratory findings in PF are the same as in overt disseminated intravascular coagulation, with most patients demonstrating thrombocytopenia, elevated D-dimer or fibrin split products, hypofibrinogenemia, and prolonged PT ± aPTT (Table 1); levels of PC, PS, and antithrombin are typically very low.
Evaluation and management
PF is a medical emergency, with a mortality of ~50%.4 In patients with suspected PF, the evaluation must proceed expeditiously and coagulation-targeted treatment initiated early (Table 2). Consultation with a dermatologist can be helpful in identifying skin findings characteristic of PF, although a skin biopsy is not required to establish the diagnosis. Patients with suspected acute infectious PF should be empirically treated with broad-spectrum antibiotics to cover N meningitidis, S pneumoniae, gram-negative rods, and methicillin-resistant S aureus until a culprit microorganism is identified. Some patients may ultimately require limb amputation due to persistence of gangrenous, necrotic tissue.5
Massachusetts General Hospital pathway for treatment of infectious purpura fulminans
| Days of presentation | Laboratory monitoring | Treatment | ||||
|---|---|---|---|---|---|---|
| Intravenous UFH | FFP | Cryoprecipitate | PC replacement | Antithrombin concentrate | ||
| 0-3 | • Complete blood count • D-dimer or fibrin split products • Fibrinogen • PT and aPTT • Anti-Xa (while on UFH) • Antithrombin, PC, and PS activities | 80 U/kg bolus followed by 18 U/kg/h, targeting anti-Xa 0.3-0.7 U/mL | 2 units followed by 1 unit every 4 hours | 10 units, targeting fibrinogen ≥100 mg/dL | PC concentrate 100 U/kg or prothrombin complex concentrate 25-50 U/kg, targeting PC activity >80% | 85 U/kg, targeting antithrombin activity >80% |
| 4-5 | 1 unit every 6 hours | |||||
| 6-7 | 1 unit every 8 hours | |||||
| • Consider intravenous vitamin K 5 mg at the time of presentation • In patients on anticoagulation, platelets may be transfused to maintain platelet count ≥30 000/µL, but platelets should not be transfused in absence of anticoagulation or bleeding | ||||||
| • For acute infectious purpura fulminans: broad-spectrum antibiotics with coverage against Neisseria meningitidis and other encapsulated organisms as well as methicillin-resistant Staphylococcus aureus until a culprit microorganism is identified | ||||||
| Days of presentation | Laboratory monitoring | Treatment | ||||
|---|---|---|---|---|---|---|
| Intravenous UFH | FFP | Cryoprecipitate | PC replacement | Antithrombin concentrate | ||
| 0-3 | • Complete blood count • D-dimer or fibrin split products • Fibrinogen • PT and aPTT • Anti-Xa (while on UFH) • Antithrombin, PC, and PS activities | 80 U/kg bolus followed by 18 U/kg/h, targeting anti-Xa 0.3-0.7 U/mL | 2 units followed by 1 unit every 4 hours | 10 units, targeting fibrinogen ≥100 mg/dL | PC concentrate 100 U/kg or prothrombin complex concentrate 25-50 U/kg, targeting PC activity >80% | 85 U/kg, targeting antithrombin activity >80% |
| 4-5 | 1 unit every 6 hours | |||||
| 6-7 | 1 unit every 8 hours | |||||
| • Consider intravenous vitamin K 5 mg at the time of presentation • In patients on anticoagulation, platelets may be transfused to maintain platelet count ≥30 000/µL, but platelets should not be transfused in absence of anticoagulation or bleeding | ||||||
| • For acute infectious purpura fulminans: broad-spectrum antibiotics with coverage against Neisseria meningitidis and other encapsulated organisms as well as methicillin-resistant Staphylococcus aureus until a culprit microorganism is identified | ||||||
UFH, unfractionated heparin.
Therapeutic anticoagulation and plasma transfusion support are critical components in managing PF (Table 2). At our institutions, we favor immediate administration of 2 units fresh-frozen plasma (FFP) followed by 1 unit every 4 hours in patients who are able to tolerate such a volume load in order to replenish endogenous anticoagulants; if available, plasma-derived PC and antithrombin concentrates should be given in conjunction with FFP, targeting PC and antithrombin activities of ≥80%.1 Simultaneously, we initiate therapeutic anticoagulation with intravenous heparin, administering an initial bolus of 80 U/kg followed by a continuous infusion of 18 U/kg with dose adjustment to maintain an anti-Xa level of 0.3 to 0.7 U/mL. We transfuse cryoprecipitate to maintain a fibrinogen >100 mg/dL while on anticoagulation. Neither thrombocytopenia nor a prolonged PT or aPTT is an absolute contraindication to anticoagulation in PF due to the prothrombotic nature of the disease, and the decision to withhold anticoagulation should be made on a case-by-case basis. Vitamin K should also be given to correct factor deficits that may contribute to coagulopathy. The use of therapeutic plasma exchange or intravenous immunoglobulin is described in case reports, although their exact benefit is uncertain.1 The role for long-term anticoagulation or antiplatelet therapy after discharge remains unclear. We advise patients with PF to maintain up-to-date vaccination against all encapsulated organisms and to seek prompt medical attention in the event of an infectious exposure such as an animal bite or contact with a known case of meningococcal meningitis.
CLINICAL CASE 1 (Continued)
The patient's laboratory testing returns with PC activity of 5%, PS activity of 15%, and antithrombin activity of 47%. He is diagnosed with acute infectious PF and initiated on intravenous heparin alongside concomitant FFP transfusions. PC and antithrombin concentrates are infused repeatedly until daily laboratory studies show recovery of PC and antithrombin activities ≥80%. He is given 1 dose of intravenous vitamin K 5 mg on admission and treated with broad antimicrobial coverage. Over the course of his 65-day hospitalization, he gradually improves, with involvement of the surgical and wound care services. He is discharged on long-term anticoagulation with warfarin.
CLINICAL CASE 2
A 52-year-old woman with stage IV melanoma and bony metastases is admitted for acute-onset dyspnea. Physical examination reveals tachycardia and asymmetric enlargement of the right calf. Laboratory studies show a hemoglobin of 10.2 g/dL and platelet count of 28 000/μL. A computed tomography and angiography study of the chest demonstrates acute bilateral pulmonary emboli (PE) in the segmental vessels of the right and left upper lung lobes. A Doppler ultrasound of the right lower extremity shows an extensive deep venous thrombosis (DVT) in the right femoral vein extending to the popliteal vein. The hematology service is consulted for recommendations regarding anticoagulation management in the context of severe thrombocytopenia.
Question 2: How do we manage anticoagulation therapy in patients with cancer-associated thrombosis with thrombocytopenia?
Pathophysiology
From its earliest descriptions in the form of Trousseau syndrome, the hypercoagulability of malignancy has been postulated to arise as a consequence of numerous hemostatic derangements, including the production of tissue factor by tumor cells and tumor-derived microvesicles, activation of platelets and endothelial cells, release of inflammatory cytokines, impairment of fibrinolysis by plasminogenactivator inhibitor-1, and production of the cysteine protease cancer procoagulant.6 A number of tumor- and host-specific factors may increase the risk of cancer- associated thrombosis (CAT), including tumor type, patient age, body mass index, blood count parameters, antineoplastic therapy, and central venous catheters. Many of these factors have been incorporated into various CAT risk scores (eg, Khorana, Vienna CATS, CATSCORE) that assess the probability of developing CAT, although the predictive accuracy of these scores has been debated.7
Thrombocytopenia, part of the Khorana score, is common in cancer, affecting up to 80% of patients depending on cancer type and treatment.8 Thrombocytopenia in cancer may arise from numerous etiologies (Table 3) and is associated with increased rates of both thrombosis and bleeding in patients with cancer, complicating the management of CAT.9,10 The problem is particularly prevalent in the inpatient setting, where thrombosis rates are 2-fold higher in hospitalized patients with cancer compared to those without, and 2.1% of hospitalized patients with cancer experience major or clinically relevant bleeding.11,12
Causes of thrombocytopenia in cancer
| Direct effect of cancer | • Bone marrow infiltration leading to myelophthisis • Splenic infiltration leading to hypersplenism |
| Antineoplastic treatments and other medications | • Cytotoxic chemotherapy • Targeted therapy • Radiation therapy • Antibiotics |
| Microangiopathic disorders | • DIC • Thrombotic microangiopathy |
| Immune-mediated disorders | • HIT • ITP |
| Systemic or other factors | • Infection or sepsis • Liver disease • Thrombosis • Critical illness |
| Direct effect of cancer | • Bone marrow infiltration leading to myelophthisis • Splenic infiltration leading to hypersplenism |
| Antineoplastic treatments and other medications | • Cytotoxic chemotherapy • Targeted therapy • Radiation therapy • Antibiotics |
| Microangiopathic disorders | • DIC • Thrombotic microangiopathy |
| Immune-mediated disorders | • HIT • ITP |
| Systemic or other factors | • Infection or sepsis • Liver disease • Thrombosis • Critical illness |
Adapted from Liebman.10
DIC, disseminated intravascular coagulation; HIT, heparin-induced thrombocytopenia; ITP, immune thrombocytopenia.
Evaluation and management
The decision to anticoagulate patients with CAT and thrombocytopenia must weigh the competing risks of thrombus progression or recurrence in the absence of anticoagulation vs bleeding with anticoagulation.13 Outside of malignancy, segmental PE and proximal lower extremity DVT are viewed as higher-risk thrombotic events than subsegmental PE or distal lower extremity DVT, respectively, although in the context of active cancer, these events all pose similar recurrence risks and warrant consideration of anticoagulation.13,14 The Ottawa score, comprising sex, cancer type and stage, and prior venous thromboembolism, was designed to predict recurrent venous thromboembolism risk in CAT during the first 6 months of anticoagulation therapy, although its reliability varies across different published studies.15 Bleeding risk in CAT is dependent on cancer type, tumor location, and thrombocytopenia severity and duration and may be further increased by older age, concomitant infection, liver or renal disease, a history of inherited and/or acquired coagulation or platelet function abnormalities, prior hematopoietic stem cell transplant, or a bleeding history.9 Both time-varying and time-invariant contributors to the natural history of CAT recurrence and bleeding risk are considered in formulating decisions about anticoagulation management, reflected in a shared decision-making process with the patient in consideration of their values and preferences.
For patients with CAT and thrombocytopenia in whom anticoagulation is indicated, 2 management strategies are commonly practiced, both endorsed in consensus guidelines from the National Comprehensive Cancer Network (Figure 2).9,16 The first is to administer full-dose anticoagulation with platelet transfusions to maintain a platelet count of 40 000 to 50 000/µL. The second avoids platelet transfusions and uses full-dose anticoagulation with platelet counts >50 000/µL, partial-dose anticoagulation with platelet counts of 25 000 to 50 000/µL, and no anticoagulation with platelets <25 000/µL.17,18 The first approach has historically been more common, yet evidence to support this has been generally lacking and is the subject of ongoing research. Recently, a prospective multicenter study (TROVE) evaluated outcomes in patients with CAT and thrombocytopenia treated with (1) full-dose anticoagulation and platelet transfusion support, (2) modified-dose anticoagulation without platelet transfusions, or (3) no anticoagulation19 ; for each patient, the specific anticoagulation strategy selected was left to discretion of the treating clinician. The median platelet counts were 65 000/µL for patients receiving full-dose anticoagulation with platelet transfusions, 37 000/µL for modified-dose anticoagulation, and 16 000/µL for no anticoagulation. Patients treated with full-dose anticoagulation and platelet transfusions had slightly higher risks of recurrent venous thromboembolism and major bleeding compared to those treated with dose-modified anticoagulation without platelet transfusions. The study was limited by a lack of randomization for treatment allocation and differences in some baseline characteristics among treatment groups. Nonetheless, the TROVE study represents an important advance in the treatment of CAT as the first multicenter, observational, prospective study to demonstrate support for dose-modified anticoagulation based on platelet count.
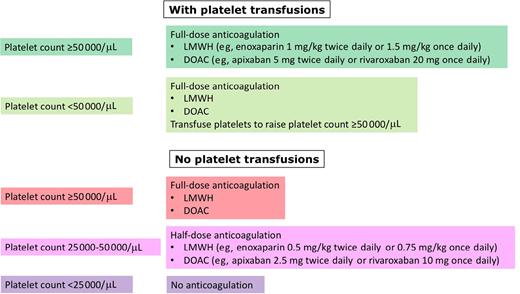
Anticoagulation management in patients with CAT and thrombocytopenia. DOAC, direct oral anticoagulant; LMWH, low-molecular-weight heparin.
Anticoagulation management in patients with CAT and thrombocytopenia. DOAC, direct oral anticoagulant; LMWH, low-molecular-weight heparin.
CLINICAL CASE 2 (Continued)
The patient undergoes a thorough evaluation for thrombocytopenia, which reveals marrow infiltration by melanoma. Her bleeding history does not raise suspicion for an underlying bleeding diathesis. Her creatinine, transaminases, and fibrinogen levels are all normal. Magnetic resonance imaging of the brain shows no metastases. Following a shared decision- making discussion with the patient and her other providers, she is recommended for modified anticoagulation with enoxaparin at a reduced dose of 0.5 mg/kg twice daily and close monitoring for signs and symptoms of progressive thrombosis or bleeding.
CLINICAL CASE 3
A 57-year-old man is hospitalized for fever and dyspnea. His presenting oxygen saturation is 90% on room air. Testing for severe acute respiratory syndrome coronavirus 2 (coronavirus disease 2019 [COVID-19]) is positive. Chest imaging shows diffuse lung infiltrates. He receives supplemental oxygen via nasal cannula at a rate of 3 L/min, is given tocilizumab, and is started on prophylactic-dose enoxaparin (40 mg daily). A D-dimer level on admission is elevated to 2.31 mg/L FEU (normal range, ≤0.55 mg/L FEU). Two days later, his oxygenation worsens; his supplemental oxygen is increased to 6 L/min. His D-dimer rises markedly to 33.8 mg/L fibrinogen equivalent units (FEU). A computed tomography and angiography study of the chest shows progression of bilateral lung infiltrates with no evidence of PE. Doppler ultrasounds of the bilateral lower extremities show no DVT. The hematology service is consulted regarding whether to empirically increase his enoxaparin dose or to add aspirin.
Question 3: How do we manage antithrombotic therapy in hospitalized patients with COVID-19?
Pathophysiology
From the earliest reports of peripheral ischemia and pulmonary microembolism at the beginning of the pandemic, COVID-19 has been viewed as a hypercoagulable disease, although the exact magnitude of this hypercoagulability in comparison to other infections has been subject to debate. Observational data from early in the pandemic suggested increased rates of PE and DVT in hospitalized patients with COVID-19 compared with historical numbers in other diseases, while more recent thrombotic rates are lower than earlier numbers.20,21 It is unclear if these differences reflect variations in hospital practices, study methods, or thrombogenicity of the virus over time.
The proposed mechanisms underlying the hypercoagulability of COVID-19 include endotheliopathy, complement activation, neutrophil activation and NETosis, platelet and monocyte activation, fibrinolytic derangements, ADAMTS13 depletion, antiphospholipid antibody production, and other immunothrombotic mechanisms along with virus-specific factors.22-27 An elevated D-dimer, a hallmark of COVID-19-associated coagulopathy, is not specific to venous or arterial thromboembolism and may also be seen with bleeding or critical illness in COVID-19.28
Evaluation and management
Since 2021, several randomized controlled trials have evaluated the safety and efficacy of therapeutic-dose anticoagulation in hospitalized patients with COVID-19 (Table 4).29-33 The trial outcomes differed depending on the state of critical illness; in non–critically ill patients, therapeutic-dose anticoagulation was associated with improved mortality, organ support- or ventilator-free days, thrombosis, and other composite outcomes over standard thromboprophylaxis, while in critically ill patients, therapeutic-dose anticoagulation offered no such benefits. In some but not all trials, therapeutic-dose anticoagulation was associated with a reduction in thrombotic complications at the expense of an increase in bleeding. The studies varied in their inclusion criteria, outcome measures, and types of anticoagulation, with some trials (REMAP-CAP, ACTIV-4a, ATTAC, and HEP-COVID) using both intermediate- and prophylactic-dose anticoagulation as the comparator standard of care, complicating interpretation.
Summary of randomized controlled trial of intermediate- and therapeutic-dose anticoagulation or antiplatelet therapy in hospitalized patients with COVID-19
| Trial | Number of patients analyzed | Antithrombotic therapies | Thrombosis | Bleeding | Mortality | Primary outcome |
|---|---|---|---|---|---|---|
| (A) Inpatient therapeutic- vs prophylactic- or intermediate-dose anticoagulation | ||||||
| Critically ill patients | ||||||
| Multiplatform: REMAP-CAP, ACTIV-4a, and ATTAC30 Trial included only critically ill patients | 1098 | Therapeutic- vs prophylactic- or intermediate-dose enoxaparin (48.9%) or dalteparin (32.3%) | ⇓ Any thrombotic events: 7.2% vs 11.1% Major thrombotic events: 6.4% vs 10.4% | ⇑ Major bleeding: 3.8% vs 2.3%, OR 1.48 (0.75-3.04) | ⇔ Death in-hospital: 37.3% vs 35.5% | ⇔ Organ support-free days: OR 0.83 (0.67-1.03) |
| HEP-COVID33 Trial included patients with D-dimer >4 times ULN (98.4% adherence) with both ICU (32.8%) and non-ICU (67.2%) patients | 83 Overall study included 83 ICU and 170 non-ICU patients | Therapeutic- enoxaparin vs prophylactic- or intermediate-dose enoxaparin | ⇔ Venous and arterial thrombosis: 51.1% vs 55.3%, RR 0.92 (0.62-1.39) | ⇔ Major bleeding: 8.9% vs 0%, RR 7.62 (0.42-137.03) | ⇔ Death, overall study (both ICU and non-ICU patients): 19.4% vs 25.0%, RR 0.78 (0.49-1.23) | ⇔ Thrombosis (see other column) |
| Non–critically ill patients | ||||||
| Multiplatform: REMAP-CAP, ACTIV-4a, and ATTAC29 Trial included only non– critically ill patients | 2219 | Therapeutic- vs prophylactic- or intermediate-dose enoxaparin (69.5%) or dalteparin (7.4%) | ⇓ Major thrombotic events: 1.1% vs 2.1% | ⇑ Major bleeding:1.9% vs 0.9%, OR 1.8 (0.9-3.74) | ⇔ Death in-hospital 7.3% vs 8.2% | ⇔ Organ support-free days: OR 1.27 (1.03-1.58) High D-dimer (≥2 times ULN): OR 1.31 (1.00-1.76) Low D-dimer: OR 1.22 (0.93-1.57) Unknown D-dimer: 1.32 (1.00-1.86) |
| ACTION31 Trial included 93.7% clinically stable and 6.3% clinically unstable (ie, critically ill) patients | 614, including 576 clinically stable and 39 clinically unstable | Therapeutic-dose rivaroxaban vs prophylactic-dose enoxaparin or UFH | ⇔ Venous and arterial thrombosis: 7% vs 10%, RR 0.75 (0.45-1.26) | ⇑ Major and clinically relevant nonmajor bleeding: 8% vs 2%, RR 3.64 (1.61-8.27) | ⇔ Death: 11% vs 8%, RR 1.49 (0.90-2.46) | ⇔ Composite of time to death, duration of hospitalization, and duration of supplemental oxygen use: 34.8% vs 41.3% (win ratio 0.86, 0.59-1.22) |
| RAPID32 Trial included patients with D-dimer >ULN (97.7% adherence) | 443 | Therapeutic- vs prophylactic-dose enoxaparin (79.8%), dalteparin (10.8%), or UFH (3.7%) | ⇔ Venous thrombosis: 0.9% vs 2.5%, OR 0.34 (0.07-1.71) | ⇔ Major bleeding: 0.9% vs 1.7%, OR 0.52 (0.09-2.85) | ⇓ Death from any cause: 1.8% vs 7.6%, OR 0.22 (0.07-0.65) | ⇔ Composite of ICU admission, noninvasive or invasive mechanical ventilation, or death: 16.2% vs 21.9%, OR 0.69 (0.43-1.10) |
⇑ Mean ventilator-free days: 26.5 vs 24.7, OR 1.77 (1.02-3.08) | ||||||
| HEP-COVID33 Trial included patients with D-dimer >4 times ULN (98.4% adherence) with both ICU (32.8%) and non-ICU (67.2%) patients | 170 Overall study included 83 ICU and 170 non-ICU patients | Therapeutic- enoxaparin vs prophylactic- or intermediate-dose enoxaparin | ⇓ Venous and arterial thrombosis: 16.7% vs 36.1%, RR 0.46 (0.27-0.81) | ⇔ Major bleeding: 2.4% vs 2.3%, RR 1.02 (0.15-7.10) | ⇔ Death, overall study (both ICU and non-ICU patients): 19.4% vs 25.0%, RR 0.78 (0.49-1.23) | Thrombosis (see other column) |
| (B) Inpatient intermediate- vs prophylactic-dose anticoagulation | ||||||
| INSPIRATION34 Trial included only critically ill patients | 562 | Intermediate- vs prophylactic-dose enoxaparin | ⇔ Venous thrombosis: 3.3% vs 3.5%, OR 0.93 (0.37-2.32) | ⇔ Major and clinically relevant nonmajor bleeding: 6.2% vs 3.1%, OR 2.02 (0.89-4.61) | ⇔ All-cause mortality: 43.1% vs 40.9%, OR 1.09 (0.78-1.53) | ⇔ Composite of venous or arterial thrombosis, treatment with extracorporeal membrane oxygenation, or all-cause mortality: 45.7% vs 44.1%, OR 1.06 (0.76-1.48) |
| Perepu et al35 Trial included ICU (62.2%) and non-ICU (37.8%) patients | 169 | Intermediate- vs prophylactic-dose enoxaparin | ⇔ Venous thrombosis: 7% vs 8%, OR 1.79 (0.51-6.25) Arterial thrombosis: 3% vs 6%, OR 1.69 (0.39-7.29) | ⇔ Major bleeding: 2% vs 2%, OR 0.99 (0.14-7.14) Minor bleeding: 7% vs 7%, OR 0.99 (0.31-3.23) | ⇔ All-cause mortality: 21% vs 15%, OR 0.66 (0.30-1.45) All-cause mortality adjusted for age, sex, body mass index, and ICU admission: OR 0.53 (0.25-1.13) | ⇔ All-cause mortality (see other column) |
| (C) Postdischarge thromboprophylaxis | ||||||
| MICHELLE36 Trial included ICU (52%) and non-ICU (48%) patients | 318 | Rivaroxaban 10 mg for 35 days initiated at hospital discharge vs no postdischarge thromboprophylaxis | ⇓ Symptomatic or fatal venous thrombosis: 0.63% vs 5.03%, RR 0.13 (0.02-0.99) | ⇔ Major, clinically relevant nonmajor, and other bleeding: 2.51% vs 1.89% | ⇔ 28-day mortality: 17% vs 17%, RR 0.96 (0.89-1.04) | ⇔ Composite outcome of venous or arterial thrombosis or cardiovascular death at day 35 after hospital discharge: 3.14% vs 9.43%, RR 0.33 (0.13-0.90) |
| (D) Inpatient antiplatelet vs no antiplatelet therapy | ||||||
| RECOVERY38 Trial included patients who required no ventilation or simple oxygen (67%), noninvasive ventilation (28.1%), or invasive mechanical ventilation (4.9%) | 14747 | Aspirin 150 mg vs no antiplatelet therapy | ⇓ Venous or arterial thrombotic event: 4.6% vs 5.3%, RR 0.88 (0.76-1.01) | ⇑ Major bleeding: 1.6% vs 1.0%, OR 1.55 (1.16-2.07) | ⇔ 28-day mortality: 17% vs 17%, RR 0.96 (0.89-1.04) | ⇔ 28-day mortality (see other column) |
⇑ Discharge from hospital within 28 days: 75% vs 74%, RR 1.06 (1.02-1.10) | ||||||
| ACTIV-4a39 Trial included patients with D-dimer ≥2 times ULN or age 60-80 years | 562 | Therapeutic-dose UFH + P2Y12 inhibitor (ticagrelor, 63.2%; or clopidogrel, 36.8%) vs therapeutic-dose UFH | ⇓ Any thrombotic event: 3.1% vs 1.9% | ⇔ Major bleeding: 2.0% vs 0.7%, OR 3.31 (0.64-17.2) | ⇔ In-hospital death: 4.4% vs 3.0% | ⇔ Organ support-free days: 21 vs 21, OR 0.83 (0.55-1.25) |
| REMAP-CAP40 Trial enrolled only critically ill patients | 1532 | Aspirin vs P2Y12 inhibitor (clopidogrel, 88.5%; ticagrelor, 1.3%; or prasugrel, 1.3%) vs no antiplatelet therapy | ⇔/⇓ Any thrombotic event: 12.4% vs 9.8% vs 12.7% | ⇑ Major bleeding: 2.0% vs 2.3% vs 0.4% | ⇓ In-hospital death: 28.6% vs 28.4% vs 32.1% | ⇔ Organ support-free days: 563 vs 448 vs 521 |
⇑ Hospital survival: all antiplatelet therapy, OR 1.27 (0.99-1.62) Hospital survival: all antiplatelet therapy with less than therapeutic-dose anticoagulation, OR 1.33 (0.99-1.79) Survival over 90 days: all antiplatelet therapy, HR 1.22 (1.06-1.40) | ||||||
| Trial | Number of patients analyzed | Antithrombotic therapies | Thrombosis | Bleeding | Mortality | Primary outcome |
|---|---|---|---|---|---|---|
| (A) Inpatient therapeutic- vs prophylactic- or intermediate-dose anticoagulation | ||||||
| Critically ill patients | ||||||
| Multiplatform: REMAP-CAP, ACTIV-4a, and ATTAC30 Trial included only critically ill patients | 1098 | Therapeutic- vs prophylactic- or intermediate-dose enoxaparin (48.9%) or dalteparin (32.3%) | ⇓ Any thrombotic events: 7.2% vs 11.1% Major thrombotic events: 6.4% vs 10.4% | ⇑ Major bleeding: 3.8% vs 2.3%, OR 1.48 (0.75-3.04) | ⇔ Death in-hospital: 37.3% vs 35.5% | ⇔ Organ support-free days: OR 0.83 (0.67-1.03) |
| HEP-COVID33 Trial included patients with D-dimer >4 times ULN (98.4% adherence) with both ICU (32.8%) and non-ICU (67.2%) patients | 83 Overall study included 83 ICU and 170 non-ICU patients | Therapeutic- enoxaparin vs prophylactic- or intermediate-dose enoxaparin | ⇔ Venous and arterial thrombosis: 51.1% vs 55.3%, RR 0.92 (0.62-1.39) | ⇔ Major bleeding: 8.9% vs 0%, RR 7.62 (0.42-137.03) | ⇔ Death, overall study (both ICU and non-ICU patients): 19.4% vs 25.0%, RR 0.78 (0.49-1.23) | ⇔ Thrombosis (see other column) |
| Non–critically ill patients | ||||||
| Multiplatform: REMAP-CAP, ACTIV-4a, and ATTAC29 Trial included only non– critically ill patients | 2219 | Therapeutic- vs prophylactic- or intermediate-dose enoxaparin (69.5%) or dalteparin (7.4%) | ⇓ Major thrombotic events: 1.1% vs 2.1% | ⇑ Major bleeding:1.9% vs 0.9%, OR 1.8 (0.9-3.74) | ⇔ Death in-hospital 7.3% vs 8.2% | ⇔ Organ support-free days: OR 1.27 (1.03-1.58) High D-dimer (≥2 times ULN): OR 1.31 (1.00-1.76) Low D-dimer: OR 1.22 (0.93-1.57) Unknown D-dimer: 1.32 (1.00-1.86) |
| ACTION31 Trial included 93.7% clinically stable and 6.3% clinically unstable (ie, critically ill) patients | 614, including 576 clinically stable and 39 clinically unstable | Therapeutic-dose rivaroxaban vs prophylactic-dose enoxaparin or UFH | ⇔ Venous and arterial thrombosis: 7% vs 10%, RR 0.75 (0.45-1.26) | ⇑ Major and clinically relevant nonmajor bleeding: 8% vs 2%, RR 3.64 (1.61-8.27) | ⇔ Death: 11% vs 8%, RR 1.49 (0.90-2.46) | ⇔ Composite of time to death, duration of hospitalization, and duration of supplemental oxygen use: 34.8% vs 41.3% (win ratio 0.86, 0.59-1.22) |
| RAPID32 Trial included patients with D-dimer >ULN (97.7% adherence) | 443 | Therapeutic- vs prophylactic-dose enoxaparin (79.8%), dalteparin (10.8%), or UFH (3.7%) | ⇔ Venous thrombosis: 0.9% vs 2.5%, OR 0.34 (0.07-1.71) | ⇔ Major bleeding: 0.9% vs 1.7%, OR 0.52 (0.09-2.85) | ⇓ Death from any cause: 1.8% vs 7.6%, OR 0.22 (0.07-0.65) | ⇔ Composite of ICU admission, noninvasive or invasive mechanical ventilation, or death: 16.2% vs 21.9%, OR 0.69 (0.43-1.10) |
⇑ Mean ventilator-free days: 26.5 vs 24.7, OR 1.77 (1.02-3.08) | ||||||
| HEP-COVID33 Trial included patients with D-dimer >4 times ULN (98.4% adherence) with both ICU (32.8%) and non-ICU (67.2%) patients | 170 Overall study included 83 ICU and 170 non-ICU patients | Therapeutic- enoxaparin vs prophylactic- or intermediate-dose enoxaparin | ⇓ Venous and arterial thrombosis: 16.7% vs 36.1%, RR 0.46 (0.27-0.81) | ⇔ Major bleeding: 2.4% vs 2.3%, RR 1.02 (0.15-7.10) | ⇔ Death, overall study (both ICU and non-ICU patients): 19.4% vs 25.0%, RR 0.78 (0.49-1.23) | Thrombosis (see other column) |
| (B) Inpatient intermediate- vs prophylactic-dose anticoagulation | ||||||
| INSPIRATION34 Trial included only critically ill patients | 562 | Intermediate- vs prophylactic-dose enoxaparin | ⇔ Venous thrombosis: 3.3% vs 3.5%, OR 0.93 (0.37-2.32) | ⇔ Major and clinically relevant nonmajor bleeding: 6.2% vs 3.1%, OR 2.02 (0.89-4.61) | ⇔ All-cause mortality: 43.1% vs 40.9%, OR 1.09 (0.78-1.53) | ⇔ Composite of venous or arterial thrombosis, treatment with extracorporeal membrane oxygenation, or all-cause mortality: 45.7% vs 44.1%, OR 1.06 (0.76-1.48) |
| Perepu et al35 Trial included ICU (62.2%) and non-ICU (37.8%) patients | 169 | Intermediate- vs prophylactic-dose enoxaparin | ⇔ Venous thrombosis: 7% vs 8%, OR 1.79 (0.51-6.25) Arterial thrombosis: 3% vs 6%, OR 1.69 (0.39-7.29) | ⇔ Major bleeding: 2% vs 2%, OR 0.99 (0.14-7.14) Minor bleeding: 7% vs 7%, OR 0.99 (0.31-3.23) | ⇔ All-cause mortality: 21% vs 15%, OR 0.66 (0.30-1.45) All-cause mortality adjusted for age, sex, body mass index, and ICU admission: OR 0.53 (0.25-1.13) | ⇔ All-cause mortality (see other column) |
| (C) Postdischarge thromboprophylaxis | ||||||
| MICHELLE36 Trial included ICU (52%) and non-ICU (48%) patients | 318 | Rivaroxaban 10 mg for 35 days initiated at hospital discharge vs no postdischarge thromboprophylaxis | ⇓ Symptomatic or fatal venous thrombosis: 0.63% vs 5.03%, RR 0.13 (0.02-0.99) | ⇔ Major, clinically relevant nonmajor, and other bleeding: 2.51% vs 1.89% | ⇔ 28-day mortality: 17% vs 17%, RR 0.96 (0.89-1.04) | ⇔ Composite outcome of venous or arterial thrombosis or cardiovascular death at day 35 after hospital discharge: 3.14% vs 9.43%, RR 0.33 (0.13-0.90) |
| (D) Inpatient antiplatelet vs no antiplatelet therapy | ||||||
| RECOVERY38 Trial included patients who required no ventilation or simple oxygen (67%), noninvasive ventilation (28.1%), or invasive mechanical ventilation (4.9%) | 14747 | Aspirin 150 mg vs no antiplatelet therapy | ⇓ Venous or arterial thrombotic event: 4.6% vs 5.3%, RR 0.88 (0.76-1.01) | ⇑ Major bleeding: 1.6% vs 1.0%, OR 1.55 (1.16-2.07) | ⇔ 28-day mortality: 17% vs 17%, RR 0.96 (0.89-1.04) | ⇔ 28-day mortality (see other column) |
⇑ Discharge from hospital within 28 days: 75% vs 74%, RR 1.06 (1.02-1.10) | ||||||
| ACTIV-4a39 Trial included patients with D-dimer ≥2 times ULN or age 60-80 years | 562 | Therapeutic-dose UFH + P2Y12 inhibitor (ticagrelor, 63.2%; or clopidogrel, 36.8%) vs therapeutic-dose UFH | ⇓ Any thrombotic event: 3.1% vs 1.9% | ⇔ Major bleeding: 2.0% vs 0.7%, OR 3.31 (0.64-17.2) | ⇔ In-hospital death: 4.4% vs 3.0% | ⇔ Organ support-free days: 21 vs 21, OR 0.83 (0.55-1.25) |
| REMAP-CAP40 Trial enrolled only critically ill patients | 1532 | Aspirin vs P2Y12 inhibitor (clopidogrel, 88.5%; ticagrelor, 1.3%; or prasugrel, 1.3%) vs no antiplatelet therapy | ⇔/⇓ Any thrombotic event: 12.4% vs 9.8% vs 12.7% | ⇑ Major bleeding: 2.0% vs 2.3% vs 0.4% | ⇓ In-hospital death: 28.6% vs 28.4% vs 32.1% | ⇔ Organ support-free days: 563 vs 448 vs 521 |
⇑ Hospital survival: all antiplatelet therapy, OR 1.27 (0.99-1.62) Hospital survival: all antiplatelet therapy with less than therapeutic-dose anticoagulation, OR 1.33 (0.99-1.79) Survival over 90 days: all antiplatelet therapy, HR 1.22 (1.06-1.40) | ||||||
HR, hazard ratio; ICU, intensive care unit; OR, odds ratio; RR, relative risk; UFH, unfractionated heparin; ULN, upper limit of normal range.
For intermediate-dose anticoagulation, 2 major randomized controlled trials have been conducted, one enrolling only critically ill patients (INSPIRATION) and the other both critically ill and non–critically ill patients.34,35 Neither trial showed any difference between intermediate- vs prophylactic-dose anticoagulation in terms of thrombosis, bleeding, or mortality.
One randomized controlled trial evaluated the utility of postdischarge thromboprophylaxis with low-dose rivaroxaban and found reductions in thrombosis and cardiovascular deaths with no increase in bleeding, although broad applicability of these findings is uncertain due to certain features of the patient population and study design.36 Select patients with high-risk features such as advanced age, cardiovascular risk factors, intensive care unit stay, or a high IMPROVE venous thromboembolism or high IMPROVE-DD venous thromboembolism score may be appropriate candidates for consideration of postdischarge thromboprophylaxis.37
Three randomized controlled trials of inpatient antiplatelet vs no antiplatelet therapy showed varied results.38-40 In 1 very large trial (RECOVERY), inpatient aspirin compared with no antiplatelet therapy led to an increase in bleeding with a mild reduction in thrombosis and no change in mortality. Other trials of antiplatelet therapy from the ACTIV-4a and REMAP-CAP study groups showed either no impact on mortality or a reduction in mortality and increase in survival, particularly with antiplatelet therapy combined with lower-than-therapeutic doses of anticoagulation.
In light of all of these findings, both the National Institutes of Health and the American Society of Hematology have issued consensus guidelines recommending that non–critically ill hospitalized patients with COVID-19 be considered for therapeutic- dose anticoagulation while critically ill patients receive prophylactic-dose anticoagulation.41 The American Society of Hematology does not endorse the use of either intermediate-dose anticoagulation or postdischarge thromboprophylaxis. No consensus group has made a formal recommendation about inpatient antiplatelet therapy.
On an individual patient level, decisions about the use of escalated antithrombotic therapy must be personalized, and neither the D-dimer nor any other laboratory marker is entirely predictive of thrombosis in COVID-19. Importantly, consensus recommendations from professional societies regarding antithrombotic therapies in COVID-19 are continually being revised in response to evolving data, and individual institutions may differ in their specific practices. As an example, at the home institution of 2 of our authors (G.G., A.I.L.), we use intermediate-dose anticoagulation despite the negative data from the INSPIRATION study due to concerns that patients enrolled in the INSPIRATION trial did not match our hospital system's demographic; we do not favor empiric therapeutic-dose anticoagulation even in non–critically ill patients due to concerns about increased bleeding risks, while we use empiric aspirin in all hospitalized patients based on the REMAP-CAP trial and our own observational data.40,42
CLINICAL CASE 3 (Continued)
The patient is deemed to be acutely but not critically ill and is therefore viewed as an appropriate candidate for therapeutic- dose anticoagulation. His enoxaparin dose is increased to 1 mg/kg twice daily. Antiplatelet therapy is not started. He is given dexamethasone and remdesivir. His oxygenation gradually improves over the course of his 31-day hospitalization. Upon discharge, his anticoagulation is stopped, and he is not given postdischarge thromboprophylaxis.
Conflict-of-interest disclosure
George Goshua: no competing financial interests to declare.
Pavan K. Bendapudi: no competing financial interests to declare.
Alfred Ian Lee: no competing financial interests to declare.
Off-label drug use
Protein C concentrate and prothrombin complex concentrate are both used routinely in purpura fulminans (first case); technically they are not FDA-approved, although they are widely accepted.
