
Abstract
Although the direct oral anticoagulants (DOACs) do not require routine monitoring and reduce bleeding compared with warfarin, there are special circumstances in which laboratory measurement or reversal of their anticoagulant effect may be indicated. The dilute thrombin time and ecarin-based assays are able to quantify dabigatran across a broad range of concentrations, but are not widely available. A normal thrombin time excludes clinically relevant levels and a normal activated partial thromboplastin time probably excludes excess levels of dabigatran. Factor Xa inhibitors may be quantified with an anti-Xa assay calibrated with drug-specific standards. A normal prothrombin time probably excludes excess levels of rivaroxaban and edoxaban, but not apixaban. Patients with minor and moderate DOAC-associated bleeding can be treated with supportive care and general hemostatic measures. Nonspecific reversal agents (eg, prothrombin complex concentrate, activated prothrombin complex concentrate) are of unproven benefit, carry a risk of thrombosis, and should be reserved for severe bleeding. Specific reversal agents, such as idarucizumab (a monoclonal antibody fragment that binds dabigatran) and andexanet alfa (a recombinant factor Xa variant that binds factor Xa inhibitors but lacks coagulant activity), are in clinical development.
Learning Objectives
Understand the interpretation of coagulation tests in patients taking a direct oral anticoagulant
Describe nonspecific and specific strategies for reversal of the direct oral anticoagulants
The direct oral anticoagulants (DOACs), dabigatran (a direct thrombin inhibitor) and rivaroxaban, apixaban, and edoxaban (direct factor Xa inhibitors), have been variably approved in the United States and other jurisdictions for prevention of stroke and systemic embolism in patients with nonvalvular atrial fibrillation, for treatment and secondary prevention of venous thromboembolism, and for prevention of venous thromboembolism after major orthopedic surgery. In large phase III trials, unmonitored treatment with DOACs was shown to be non-inferior and, in some cases, superior to dose-adjusted warfarin for the prevention of thromboembolism. Compared with warfarin, the DOACs reduced major bleeding by 28% and intracranial and fatal hemorrhage by approximately 50%.1
Although the DOACs do not require routine monitoring and reduce bleeding compared with warfarin, there are special circumstances in which laboratory measurement and/or reversal of the anticoagulant activity of a DOAC may be desired. The purpose of this review is to summarize current evidence and provide practical guidance to clinicians on laboratory measurement and reversal of DOACs.
Laboratory measurement
Liquid chromatography/tandem mass spectrometry (LC-MS/MS) is the gold standard method for measurement of plasma DOAC concentrations. Steady-state trough and peak plasma concentrations of the DOACs, as measured by LC-MS/MS, are shown in Table 1.2-5 Levels vary widely from trough to peak and among individual patients.6 For instance, peak levels of dabigatran vary by a factor of ∼7 from the 5th to the 95th percentile; trough levels of rivaroxaban vary 14.5-fold over this range.

Although limited data on the relationship between DOAC levels and clinical outcomes have been published,7 therapeutic ranges (ie, plasma levels that yield optimal clinical outcomes) have not been defined. In lieu of therapeutic ranges, we find it useful to consider the concept of the “on-therapy” range. We define the on-therapy range for a given DOAC at a given dose as the interval delineated by the 5th percentile trough concentration and the 95th percentile peak concentration. Drug levels lower than the 5th percentile trough concentration may be thought of as in the “below on-therapy” range whereas those greater than the 95th percentile peak concentration may be considered to be “above on-therapy” (Figure 1). By definition, the large majority of patients in steady-state will have drug levels that fall within the on-therapy range at any time during treatment.

Below on-therapy, on-therapy, and above on-therapy ranges for DOACs. Therapeutic ranges for the DOACs have not been established. In lieu of therapeutic ranges, we define the “on-therapy” range as the interval from the 5th percentile trough concentration to the 95th percentile peak concentration. Drug levels below this range may be regarded as “below on-therapy”, those exceeding this range as “above on-therapy”. Situations in which below or above on-therapy DOAC levels may be suspected are listed.
Below on-therapy, on-therapy, and above on-therapy ranges for DOACs. Therapeutic ranges for the DOACs have not been established. In lieu of therapeutic ranges, we define the “on-therapy” range as the interval from the 5th percentile trough concentration to the 95th percentile peak concentration. Drug levels below this range may be regarded as “below on-therapy”, those exceeding this range as “above on-therapy”. Situations in which below or above on-therapy DOAC levels may be suspected are listed.
Why measure DOAC levels?
Unlike vitamin K antagonists, the DOACs do not require routine laboratory monitoring and dose adjustment. However, measurement may be indicated in special circumstances, particularly those in which below on-therapy or above on-therapy levels are suspected (Figure 1). For example, DOAC levels in the below on-therapy range may be suspected in the setting of treatment failure or patient-specific factors, such as obesity, renal hyperfunction, or gastrointestinal malabsorption. Levels in the above on-therapy range may be suspected in the context of bleeding, overdose, or patient-specific factors associated with bioaccumulation, such as renal insufficiency, low body weight, advanced age, or drug interaction. Assessment of DOAC concentration may also be sought in a patient with trauma or need for emergent surgery or thrombolytic therapy.
Attributes of an ideal assay
To achieve accurate quantification of DOAC levels, an assay must exhibit a high degree of linearity (r2 values ≥0.9) with drug concentration, as measured by LC-MS/MS. Because it may be desirable to measure below on-therapy, on-therapy, or above on-therapy DOAC levels depending on the clinical context, an ideal assay should show linearity across a broad range of drug concentrations. The assay should also be sufficiently sensitive to the lowest clinically relevant concentrations of the drug of interest. Finally, from a practical standpoint, the assay should be readily available on a 24-7 basis because there may be an emergent indication for measurement. There is no assay for DOAC measurement that meets all of these idealized criteria. Current evidence for measurement of DOACs was evaluated in 2 recent systematic reviews8,9 and is summarized below.
Dabigatran
Thrombin time.
The thrombin time (TT) is inordinately sensitive to dabigatran. Depending on the reagent, a concentration as little as 25 ng/mL (well below the median trough of 90 ng/mL) can make the TT unmeasurable (ie, plasma will not clot after addition of thrombin).8 The TT is therefore not useful for quantification. A normal TT excludes clinically relevant drug levels.
Dilute thrombin time.
In the dilute TT, the excessive sensitivity of the TT is overcome by diluting the patient sample with normal plasma. The dilute TT exhibits a high degree of linearity with plasma dabigatran concentration across a wide range of levels (r2 0.92-0.99).8 Accuracy is diminished at levels <50-100 ng/mL. Good results have been reported with both in-house modifications of the TT and a commercially available dilute TT (HEMOCLOT, HYPHEN BioMed, Neuvillesur-Oise, France). Availability of the dilute TT is limited. In a recent survey in Australia and New Zealand, only 9 of 592 laboratories offered the assay.10
Ecarin-based assays.
Ecarin is a snake venom that cleaves prothrombin to meizothrombin, an intermediate of thrombin. The thrombin-like activity of meizothrombin is inhibited by dabigatran. This property of dabigatran forms the basis for 2 assays; the ecarin clotting time (ECT) and ecarin chromogenic assay (ECA). Both assays correlate with dabigatran concentration in a linear fashion (r2 0.92-1.00) across a broad range of levels.8 Precision may be reduced at concentrations <50 ng/mL.11 The ECT and ECA are hampered by limited availability, lack of standardization, and variability in sensitivity to dabigatran among different lots of ecarin.8
Activated partial thromboplastin time.
The dose–response relationship between the activated partial thromboplastin time (APTT) and dabigatran level is linear up to a concentration of 200-300 ng/mL and then flattens out at higher concentrations. This curvilinear relationship precludes accurate quantification of dabigatran using the APTT, particularly at higher concentrations.8
Commercial APTT reagents vary widely in their sensitivity to dabigatran. The APTT of plasma spiked with dabigatran 120 ng/mL ranged from 26.0 to 91.9 s in a study of 9 different APTT methods.12 Coagulation laboratories should perform dose–response studies using calibration standards to define the sensitivity of their APTT method to dabigatran. The APTT may not be prolonged in the presence of on-therapy trough levels, particularly if a relatively insensitive reagent is used. In 1 study of ex vivo plasma samples from patients taking dabigatran 150 mg BID, 18% of participants had a normal APTT at trough.13
Prothrombin time/international normalized ratio.
The prothrombin time/international normalized ratio (PT/INR) is less sensitive to dabigatran than the APTT and may be normal in the presence of on-therapy and even above on-therapy levels. In a study of ex vivo samples from patients with atrial fibrillation, an INR of 1.2 or greater was consistently observed only when dabigatran concentrations exceeded 400 ng/mL.11 As with the APTT, commercial PT reagents differ in their sensitivity to dabigatran. In a survey of 71 coagulation laboratories, the PT of plasma spiked to a concentration of 300 ng/mL ranged from 15.7 to 50.2 s, depending on the reagent.12
Rivaroxaban, apixaban, and edoxaban
Anti-Xa activity.
Anti-Xa activity assays calibrated with drug-specific standards (eg, a rivaroxaban anti-Xa assay calibrated with rivaroxaban-specific standards) show a high degree of linear correlation with levels of rivaroxaban (r2 0.95-1.00),8 apixaban (r2 0.89-0.97),8 and edoxaban (r2 0.96-0.99)9 over a broad range of concentrations. Precision is decreased at below and above on-therapy plasma concentrations. Use of a chromogenic anti-Xa assay calibrated with unfractionated or low molecular weight heparin is associated with a more limited range of linearity and thus a narrower interval of drug concentrations across which accurate quantification can be achieved.14 Most laboratories have not yet established rivaroxaban, apixaban, and edoxaban-specific standard curves. In a 2013 survey of coagulation laboratories, 300 centers reported performing an anti-Xa assay for measurement of heparin, but only 9 participated in quantifying rivaroxaban.15
Prothrombin time/international normalized ratio.
Rivaroxaban and edoxaban prolong the PT in a concentration-dependent manner. The PT/INR is only mildly increased and may remain in the normal range at typical trough levels. In a study of healthy volunteers, the PT increased by an average of 40% at 1.5 hours and 10% at 12 hours after ingestion of a single 60 mg dose of edoxaban.16 Thromboplastin reagents differ markedly in their sensitivity to rivaroxaban and edoxaban. In a study of samples spiked with rivaroxaban, interassay variability was reduced by use of an international sensitivity index specific for rivaroxaban but not by conversion to an INR used for monitoring warfarin.17 Sensitivity indices to direct oral factor Xa inhibitors have not been defined for most PT reagents. Laboratories should conduct dose–response studies with drug-specific standards to establish the sensitivity of their PT method to rivaroxaban and edoxaban.
The PT/INR is less sensitive to apixaban than it is to rivaroxaban and edoxaban, probably because apixaban binds to factor Xa more slowly.18 Most PT reagents have insufficient sensitivity to detect not only trough but also peak and above on-therapy levels of apixaban.
Activated partial thromboplastin time.
The APTT is less sensitive to direct oral factor Xa inhibitors than the PT/INR. A normal APTT does not exclude on-therapy drug levels. In a study comparing 10 different APTT reagents, all yielded a ratio of 1.1 times control or less when the spiked apixaban concentration was 100 ng/mL.19 In an in vitro study of plasma spiked with edoxaban, a concentration of 500 ng/mL was required to double the baseline APTT.5
Suggestions for laboratory measurement
Selection of the appropriate laboratory assay depends on the DOAC that the patient is taking and the clinical objective (Table 2).8,9 Because assays most suitable for DOAC quantification such as the dilute TT, ECT, ECA, and anti-Xa activity are not widely offered, assay availability is also an important consideration. Even in centers where these assays are available, it may be challenging to offer them on a stat basis because of the technical expertise required to perform the assays and the relatively low volume of requests.
Suggestions for laboratory measurement of DOACs
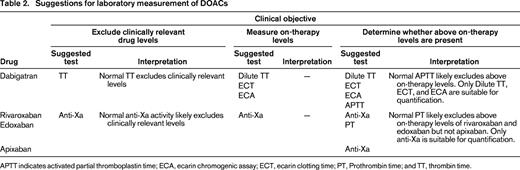
APTT indicates activated partial thromboplastin time; ECA, ecarin chromogenic assay; ECT, ecarin clotting time; PT, Prothrombin time; and TT, thrombin time.
For dabigatran, a normal TT excludes clinically relevant drug levels. The dilute TT, ECT, and ECA may be used to quantify dabigatran concentration across a broad range of levels. A normal APTT likely excludes above on-therapy levels, but not necessarily on-therapy or below on-therapy levels. The PT/INR is not useful.
For rivaroxaban, apixaban, and edoxaban, an anti-Xa assay (ideally calibrated with drug-specific standards) may be used to quantify drug concentration across a broad range of levels. A normal PT likely excludes above on-therapy levels of rivaroxaban and edoxaban, but not apixaban. The APTT is not useful due to insufficient sensitivity.
Reversal
Nonspecific reversal strategies
In lieu of clinically available specific reversal agents, prothrombin complex concentrate (PCC), activated PCC (APCC) and recombinant factor VIIa (rVIIa) have been studied for their ability to reverse the anticoagulant effect of DOACs in vitro, in animal models and in human volunteers receiving DOACs. Studies evaluating clinical outcomes in DOAC-treated patients receiving nonspecific reversal agents for bleeding complications are lacking. As a result, there is no established relationship between laboratory test correction and bleeding cessation, or other clinical outcomes. Tables 3 and 4 summarize the results of published animal model and human volunteer studies. These results should be interpreted with caution not only due to the variability of results, but also due to possible important biologic differences between DOAC-treated patients at risk of thromboembolism and experimental animals or healthy volunteer subjects.
Published studies of nonspecific agents for reversal of dabigatran anticoagulant effect in animals and humans
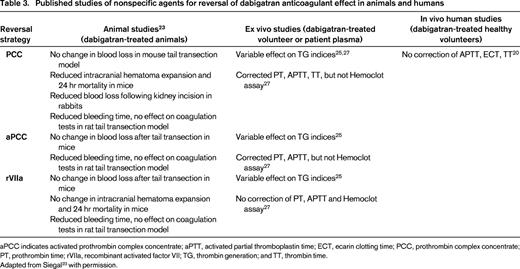
aPCC indicates activated prothrombin complex concentrate; aPTT, activated partial thromboplastin time; ECT, ecarin clotting time; PCC, prothrombin complex concentrate; PT, prothrombin time; rVIIa, recombinant activated factor VII; TG, thrombin generation; and TT, thrombin time.
Adapted from Siegal23 with permission.
Published studies of nonspecific agents for reversal of oral factor Xa inhibitor anticoagulant effect in animals and humans
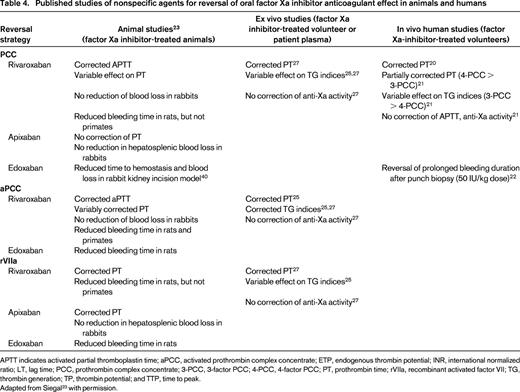
APTT indicates activated partial thromboplastin time; aPCC, activated prothrombin complex concentrate; ETP, endogenous thrombin potential; INR, international normalized ratio; LT, lag time; PCC, prothrombin complex concentrate; 3-PCC, 3-factor PCC; 4-PCC, 4-factor PCC; PT, prothrombin time; rVIIa, recombinant activated factor VII; TG, thrombin generation; TP, thrombin potential; and TTP, time to peak.
Adapted from Siegal23 with permission.
Prothrombin complex concentrate.
PCC is a plasma-derived product containing vitamin K -dependent coagulation factors II, IX and X (3-factor PCC) or II, VII, IX and X (4-factor PCC) developed for reversal of vitamin K antagonist anticoagulant (VKA) effect. In a randomized crossover study, infusion of 4-factor PCC (50 U/kg) corrected PT prolongation and abnormal endogenous thrombin potential (ETP) compared with placebo in healthy subjects receiving rivaroxaban (20 mg twice daily for 2.5 days).20 In the same study, infusion of 4-factor PCC (50 U/kg) did not correct the APTT, ECT, or TT in dabigatran-treated subjects (150 mg twice daily for 2.5 days). A recent study showed that 4-factor PCC corrected the PT to a greater extent than 3-factor PCC (2.5-3.5 seconds vs 0.6-1.0 seconds, respectively) in patients receiving rivaroxaban (20 mg twice daily for 4 days).21 Neither product corrected the APTT or anti-Xa activity. Three-factor PCC had a greater effect than 4-factor PCC on the ETP, peak thrombin generation, and time-to-peak thrombin generation, although neither concentrate influenced the abnormal lag time. A randomized study showed that 4-factor PCC (50 U/kg) reduced bleeding duration compared to placebo following punch biopsy in edoxaban-treated volunteers (60 mg single dose).22
PCC has variable effects on abnormal routine coagulation tests and thrombin generation assays induced by DOACs in vitro including correction of PT prolongation induced by edoxaban and dabigatran, some abnormal thrombin generation indices induced by dabigatran and rivaroxaban, but no effect on the Hemoclot assay (reviewed by Siegal23 ).
When administered to VKA-treated patients with bleeding complications, PCC carries a risk of thromboembolism (1.4%).24
Activated prothrombin complex concentrate.
APCC is a plasma-derived concentrate containing factors II, VII, IX, and X which are activated during the manufacturing process. It is commercially available as factor eight inhibitor bypassing activity (FEIBA, Baxter Bioscience, Vienna, Austria). In vitro, APCC has variable effects on DOAC-induced abnormal coagulation tests and thrombin generation indices (reviewed by Siegal23 ). When added to blood taken from subjects receiving rivaroxaban and dabigatran (20 and 150 mg single doses, respectively), APCC corrected abnormal thrombin generation indices.25
In hemophilia patients for whom APCC was developed, thrombotic events occurred at a rate of 4-8 events per 105 infusions with the majority of events occurring in patients with risk factors for thrombosis.26
Recombinant factor VIIa.
In vitro, rVIIa has variable effects on DOAC-induced coagulation and thrombin generation test abnormalities (reviewed by Siegal23 ). It corrected some abnormal thrombin generation indices with no correction of PT, APTT or Hemoclot assay when added ex vivo to dabigatran-treated plasma. rVIIa corrected rivaroxaban-induced prolonged PT and some abnormal thrombin generation indices with no effect on anti-Xa activity.25,27
PER977.
PER977 (Perosphere, Bedford, New York) is a small synthetic molecule that binds to several anticoagulants including DOACs via noncovalent bonding and charge–charge interactions.28 It is currently under development as a nonspecific DOAC reversal agent. Although it has not been shown to reverse DOAC-related coagulation test abnormalities in vitro, it reduced bleeding in a rivaroxaban-treated rabbit liver laceration model.29 In edoxaban-treated healthy volunteers (60 mg single dose), PER977 normalized prolonged whole-blood clotting time compared to placebo.28 A phase II study of escalating doses of PER977 in volunteers at steady-state edoxaban dosing is currently underway (clinicaltrials.gov, identifier NCT02207257).
Specific reversal agents
Idarucizumab.
Idarucizumab (anti-Dabi-Fab; Boehringer Ingelheim, Biberach, Germany) is a humanized monoclonal antibody fragment with high affinity for dabigatran undergoing clinical development as a specific antidote for dabigatran. In dabigatran-treated rats, idarucizumab showed a dose-dependent reduction in blood loss following tail transection.30 It also reduced blood loss and improved survival in dabigatran-treated pigs with blunt liver injury and dose-dependently corrected dabigatran-induced abnormal dilute TT in monkeys.31,32 In healthy volunteer subjects, idarucizumab corrected dabigatran-induced prolonged clotting times (Hemoclot, TT, APTT, ecarin clotting time, and activated clotting time).33 It also reversed the effects of dabigatran on coagulation tests in male and female volunteers of varying ages and renal function.34 The ongoing RE-VERSE AD study is a phase III case series evaluating the efficacy and safety of idarucizumab in dabigatran-treated patients requiring reversal of dabigatran anticoagulant effect for uncontrolled bleeding or urgent surgery (clinicaltrials.gov, identifier NCT02104947). A recent interim analysis reported results in 51 patients with serious bleeding and 39 patients requiring an urgent procedure. Administration of 5 g of intravenous idarucizumab resulted in rapid normalization of the dilute TT and ECT. In subjects with serious bleeding, hemostasis was restored at a median of 11.4 hours after idarucizumab injection. Normal intraoperative hemostasis was achieved in 92% of patients in the urgent procedure group.35 Idarucizumab has been submitted to the US Food and Drug Administration for approval.
Andexanet alfa.
Andexanet alfa (Portola Pharmaceuticals, San Francisco, CA) is a recombinant factor Xa protein which lacks catalytic and membrane binding activity, but retains the ability to bind factor Xa inhibitors.36 It is currently under clinical development for specific reversal of factor Xa inhibitor anticoagulant effect. In vitro studies showed dose-dependent correction of abnormal anti-Xa activity induced by rivaroxaban, apixaban, betrixaban, and edoxaban.36,37 In rats treated with rivaroxaban, apixaban, and betrixaban, andexanet corrected the international normalized ratio (INR).36 It corrected abnormal coagulation assays and reduced blood loss following liver laceration in rivaroxaban-treated rabbits.36 In healthy volunteers receiving apixaban, andexanet dose-dependently decreased anti-Xa activity compared to placebo.38 Preliminary results of a phase III study showed that andexanet reversed apixaban-induced coagulation test and thrombin generation abnormalities compared to placebo in older healthy subjects (aged 55-73) (clinicaltrials.gov, identifier NCT02207725).39 Another ongoing phase III study is evaluating the effect of andexanet on rivaroxban-induced abnormal anti-Xa activity compared to placebo in older healthy subjects (aged 50-75) (clinicaltrials.gov, identifier NCT02220725). A prospective open-label cohort study assessing the efficacy and safety of andexanet in factor Xa inhibitor-treated patients with acute major bleeding is currently enrolling (clinicaltrials.gov, identifier NCT02329327). To achieve sustained correction of laboratory abnormalities, andexanet will likely need to be administered via bolus injection followed by continuous infusion. Andexanet administration is associated with a transient increase in prothrombin fragment F1.2 and thrombin-antithrombin complexes of unknown clinical significance, which has been attributed to an interaction with tissue factor pathway inhibitor (TFPI).38
Suggested management strategy for DOAC-associated bleeding
In the absence of clinically available specific reversal therapies, supportive measures and urgent referral for procedural or surgical intervention are the mainstay of managing DOAC-associated bleeding complications (Figure 2). Initial clinical evaluation should focus on assessing hemodynamic stability, identifying the source of bleeding and risk stratifying based on degree of blood loss. Patient assessment should also include time elapsed since drug administration, renal function (particularly for dabigatran), and relevant co-medications (eg, antiplatelet therapies, cytochrome P450 3A4, or P-glycoprotein substrates). Nonspecific reversal agents (eg, PCC, APCC) should be reserved for patients who present with severe bleeding, or uncontrolled bleeding despite maximum supportive measures.

Suggested management of DOAC-associated bleeding. An algorithm for DOAC-associated bleeding is shown. Minor and moderate bleeding may be managed with general hemostatic measures and supportive care. Nonspecific reversal agents, such as PCC or activated PCC may be considered for severe bleeding. CYP3A4 indicates cytochrome P450 3A4; DIC, disseminated intravascular coagulation; and PgP, P-glycoprotein.
Suggested management of DOAC-associated bleeding. An algorithm for DOAC-associated bleeding is shown. Minor and moderate bleeding may be managed with general hemostatic measures and supportive care. Nonspecific reversal agents, such as PCC or activated PCC may be considered for severe bleeding. CYP3A4 indicates cytochrome P450 3A4; DIC, disseminated intravascular coagulation; and PgP, P-glycoprotein.
Patients with minor bleeding (eg, epistaxis, ecchymosis, menorrhagia) may be managed conservatively with emphasis on local hemostatic measures. Drug discontinuation can be considered in conjunction with assessment of underlying thromboembolic risk to establish net clinical benefit of withholding anticoagulant therapy. The short half-life and rapid onset of anticoagulant effect of DOACs may influence the decision to proceed with drug interruption.
In patients with moderate bleeding (eg, gastrointestinal bleeding), DOACs should be discontinued. Packed red blood cells and/or plasma should be transfused for actual or expected severe anemia and coagulopathy (eg, disseminated intravascular coagulation, dilutional coagulopathy), respectively. Platelet transfusion may be considered for patients receiving concomitant antiplatelet therapies.
Severe/life-threatening bleeding should be managed with life-supporting therapies and early referral for procedural or surgical intervention. Nonspecific reversal therapies (eg, PCC 50 U/kg, APCC 80 U/kg) may be considered based on limited, poor-quality evidence and potential thrombotic risk. Hemodialysis may be used to remove dabigatran, when feasible. Antifibrinolytic therapies (tranexamic acid, aminocaproic acid) and desmopressin (DDAVP) can also be considered.
Correspondence
Adam Cuker, Hospital of the University of Pennsylvania, 3 Dulles, 3400 Spruce St, Philadelphia, PA 19014; Phone: 215-615-6555; Fax: 215-615-6599; e-mail: adam.cuker@uphs.upenn.edu.
