
Abstract
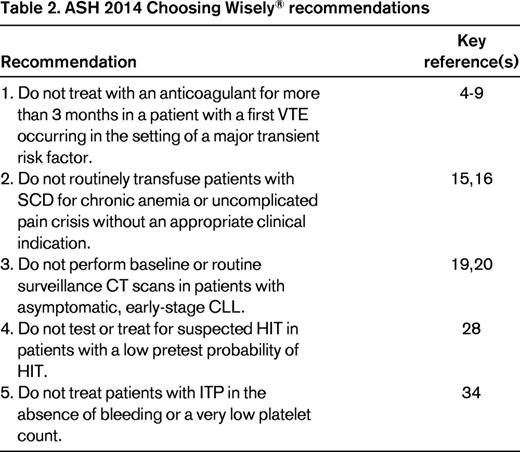
Choosing Wisely® is a medical stewardship initiative led by the American Board of Internal Medicine Foundation in collaboration with professional medical societies in the United States. The American Society of Hematology (ASH) released its first Choosing Wisely® list in 2013. Using the same evidence-based methodology as in 2013, ASH has identified 5 additional tests and treatments that should be questioned by clinicians and patients under specific, indicated circumstances. The ASH 2014 Choosing Wisely® recommendations include: (1) do not anticoagulate for more than 3 months in patients experiencing a first venous thromboembolic event in the setting of major, transient risk factors for venous thromboembolism; (2) do not routinely transfuse for chronic anemia or uncomplicated pain crises in patients with sickle cell disease; (3) do not perform baseline or surveillance computed tomography scans in patients with asymptomatic, early-stage chronic lymphocytic leukemia; (4) do not test or treat for heparin-induced thrombocytopenia if the clinical pretest probability of heparin-induced thrombocytopenia is low; and (5) do not treat patients with immune thrombocytopenia unless they are bleeding or have very low platelet counts.
Learning Objectives
To understand that the second ASH Choosing Wisely® campaign has identified 5 additional hematologic tests and treatments that should be questioned in certain circumstances
To understand duration of anticoagulation in provoked VTE, transfusion in SCD, CT scans in CLL, HIT testing, and when to treat ITP
Introduction
Choosing Wisely® is a national medical stewardship campaign led by the American Board of Internal Medicine (ABIM) Foundation in collaboration with professional medical societies. The campaign aims to encourage conversations between patients and their health care teams about tests, treatments, and procedures that, in certain scenarios, are unnecessary, can contribute to avoidable harm, and are costly. In 2012, the Institute of Medicine estimated that ∼210 billion dollars are wasted annually on unnecessary medical care in the United States,1 a daunting figure that highlights the importance of Choosing Wisely® and other stewardship initiatives.
The American Society of Hematology (ASH) released its first Choosing Wisely® list in December 2013. The list included items addressing thrombophilia testing, general RBC transfusion practices, plasma utilization for vitamin K antagonist reversal, inferior vena cava filter use for acute venous thromboembolism (VTE), and surveillance CT scans after successful treatment of aggressive lymphoma.2 This article reports the methods and results of ASH's second Choosing Wisely® campaign.
Methods
In February 2014, the ABIM Foundation decided to continue its Choosing Wisely® campaign in collaboration with interested professional societies. The ASH Choosing Wisely® Task Force was reconvened and committed to pursuing a second list. The 2014 Task Force was composed of 13 individuals representing a broad spectrum of hematologic expertise; malignant, benign, adult, and pediatric specialists were all well represented on the Task Force.
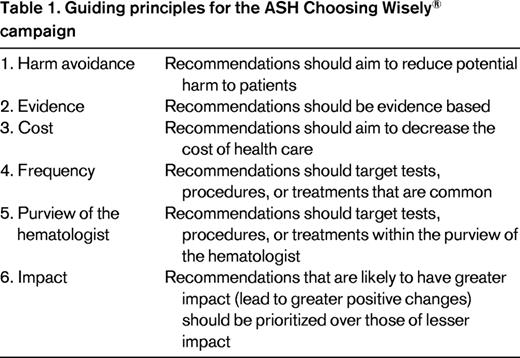
The selection and prioritization of items for ASH's second Choosing Wisely® campaign were guided by the same 5 principles used in the first campaign: (1) avoiding harm to patients, (2) producing evidence-based recommendations, (3) considering cost, (4) considering frequency of tests and treatments, and (5) making recommendations in the clinical purview of the hematologist. As with the first ASH Choosing Wisely® campaign, harm avoidance was established as the campaign's preeminent guiding principle. For the second ASH Choosing Wisely® campaign, a sixth overarching principle was adopted: impact (Table 1). Items that were felt to have a greater probability of triggering positive changes in practice were prioritized over items felt to have lower potential impact. Items that overlapped substantially with published Choosing Wisely® recommendations from other medical societies received lower priority.
Suggestions for the second ASH Choosing Wisely® list were solicited from members of the ASH Committee on Practice, the ASH Committee on Quality, the ASH Choosing Wisely® Task Force, ASH Consult-a-Colleague volunteers, and members of the ASH Practice Partnership. Guided by the 6 principles outlined above (Table 1), the ASH Choosing Wisely® Task Force scored all suggestions for inclusion in ASH's second Choosing Wisely® list. Modified group technique was used to select 10 semifinalist items.3 Systematic reviews of the literature were then completed for each of the 10 semifinalist items using the same methods described previously.2 A professional methodologist (A.E.H.) reviewed all titles and abstracts for potential inclusion. Two authors (A.E.H. and one of L.K.H., A.R., J.K., J.A.P., S.H.O., or W.A.W.) reviewed all full-text citations for eligibility. The search strategies for each of the 10 semifinalist items are outlined in the supplemental Appendix to the online Blood edition of this article. As with the first campaign, hierarchical search strategies were used such that if recent (subsequent to 2008) evidence-based guidelines were found, the literature search was curtailed.
Guided by the 6 core principles outlined in Table 1 and by our systematic reviews of the evidence, the ASH Choosing Wisely® Task Force selected 5 recommendations for inclusion in ASH's second Choosing Wisely® campaign. Each item was reviewed and revised for accuracy and clarity by 2-4 external content experts per item. The final list was reviewed and approved by the ASH executive officers and by the ABIM Foundation.
Results
A total of 210 ASH members were solicited for suggestions for ASH's second Choosing Wisely® campaign; 33 members submitted a total of 93 recommendations (16% response rate). After removing redundant items, there were 73 unique suggestions; 39 with a nonmalignant focus and 34 with a malignant focus. Among the 10 semifinalist items selected for systematic review, 7 had a nonmalignant focus and 3 had a malignant focus. One of the 10 semifinalist items was ultimately excluded because the systematic review proved to be infeasible in the prescribed time frame due to a very high number of potentially eligible citations. This item involved thrombophilia testing for arterial disease. Table 2 summarizes the 5 final recommendations of the 2014 ASH Choosing Wisely® campaign.
Discussion
The first recommendation of ASH's second Choosing Wisely® campaign is not to anticoagulate patients with a first VTE provoked by a major, transient VTE risk factor such as surgery, trauma, or an intravascular catheter for more than 3 months.4-9 Randomized controlled trials have established that there is no significant benefit to prolonged anticoagulation in the setting of major, temporary VTE risk factors.10 These recommendations are driven largely by a low risk of VTE recurrence after 3 months in the setting of a provoked VTE and are applicable to adult and pediatric patients, although the strength of the evidence is weaker for very young children.
Anticoagulation for VTE continued beyond 3 months is associated with a major bleeding risk of 2.7 per 100 patient-years with a case fatality rate of 9.1%.11 These estimates come from prospective clinical trials of warfarin; it is likely that bleeding risks are higher in clinical practice, where patients tend to be older and have more comorbidities than in trials.12 Bleeding risks may be lower with new oral anticoagulants. However, in addition to potential harms from anticoagulation, anticoagulation with new oral anticoagulants is expensive.
Importantly, the ASH Choosing Wisely® recommendation is not intended to apply to patients with non-major, transient VTE risk factors such as travel-associated immobility, pregnancy, or hormone use. Guidelines suggest that women who experience a first VTE in the setting of pregnancy should receive anticoagulation until at least 6 weeks postpartum for a minimum total duration of 3 months or longer.13 VTEs occurring in the context of exogenous estrogen use are associated with a low rate of recurrence provided that hormonal therapy/oral contraception is not resumed; 3 months of anticoagulation may be appropriate in some cases.14 However, because the optimal duration of anticoagulation has not been prospectively established for VTEs provoked by hormones or by travel, the duration of anticoagulation should be determined on a case-by-case basis.
ASH's second 2014 Choosing Wisely® recommendation advises against routine transfusion of RBCs for chronic anemia or uncomplicated pain crises in patients with sickle cell disease (SCD).15,16 Patients with SCD are uniquely vulnerable to harm from RBC transfusion. African Americans are underrepresented among the blood donor pool.17 As a result, there are important differences between the minor RBC antigens commonly represented in the donor pool and those expressed by many patients with SCD. This phenomenon, combined with recurrent exposure to blood, markedly increases the risk of alloimmunization to minor blood group antigens among patients with SCD.17 Alloimmunization can result in delayed hemolytic transfusion reactions and in difficulty finding compatible blood when necessary.
Patients with SCD are also at high risk of secondary iron overload from repeated transfusions. Iron overload is an important cause of both morbidity and mortality in patients with SCD.18 Moreover, stable patients with severe SCD typically have baseline hemoglobin values between 7 and 10 g/dL and can often tolerate 1-2 g/dL decreases in hemoglobin (often due to hemodilution after administration of intravenous fluids) without developing symptoms of anemia. There is also little evidence that episodic RBC transfusion reduces pain during acute vasoocclusive crises.16 Evidence-based guidelines on the management of SCD have recently been completed and clinicians are encouraged to refer to them for appropriate clinical indications for transfusion in patients with SCD.15
The third recommendation of ASH's 2014 Choosing Wisely® campaign advises against baseline or surveillance CT scans in patients with asymptomatic, early-stage chronic lymphocytic leukemia (CLL).19,20 Unlike in other lymphoproliferative diseases, CT scans are not necessary to fully stage patients with CLL. Both the Rai and Binet staging systems are based on physical examination findings and complete blood counts.21,22 Prognosis can be further refined with molecular tests for mutations of established prognostic significance.23 There is no evidence that baseline or surveillance CT scans improve survival in patients with asymptomatic, early-stage CLL.19,20
CT scans can also contribute to harm to patients. CTs are associated with a small, but cumulative, risk of radiation-induced malignancy.24 In addition, a recent meta-analysis estimates that 30% of CT scans detect incidental findings,25 some of which trigger further workup, exposing patients to additional risks and adding to health care costs. This phenomenon, termed the cascade effect, is well recognized in health policy literature, with most experts recommending that the best way to curtail the cascade effect is to avoid unnecessary testing in the first place.26,27
The fourth statement in this year's ASH Choosing Wisely® campaign recommends against testing or treating for heparin-induced thrombocytopenia (HIT) in patients with a low pretest probability of HIT (score of 0-3).28 The 4 Ts score is a clinical scoring system that estimates the pretest probability of HIT using readily available clinical and laboratory parameters.29 A recent meta-analysis reported that the negative predictive value of a low 4 Ts score is close to 100% in adults.30 Given that most enzyme immunoassays (EIAs) for HIT have high false-positive rates, positive EIA HIT test results in patients with low 4 Ts scores are much more likely to represent false positives than true positives. Less is known about HIT in the pediatric population, although emerging evidence suggests that HIT does occur and that overdiagnosis may be a problem in this population as well.31
Incorrectly diagnosing HIT can lead to substantial harm. Most patients tested for HIT have thrombocytopenia. Starting an alternative anticoagulant in a thrombocytopenic patient incorrectly diagnosed as having HIT exposes that patient to a risk of bleeding. Incorrectly labeling a patient as having had HIT can also result in the patient being inappropriately denied heparin in the future. Patients with cardiovascular disease, particularly those undergoing bypass surgery, have an increased incidence of both thrombocytopenia and of positive EIA HIT results.32 Due to the nature of their underlying cardiac disease, these are the same patients who are likely to require future heparin.
Finally, HIT testing increases both direct and indirect costs of care. Many hospitals use nonautomated HIT tests that require substantial technician time and thus are relatively costly laboratory tests. Confirmatory testing with serotonin release assays is also expensive due to technician time and the cost of reagents and is not performed at many hospitals. In addition, alternative anticoagulants such as argatroban are much more expensive than unfractionated heparin and in some cases are associated with higher risks of bleeding. As a result of these and other factors, it has been reported that testing for HIT is only cost-effective when the pretest probability of HIT is >8%, a number that corresponds to an intermediate or high 4 Ts score.33
ASH's final 2014 Choosing Wisely® item recommends against treating immune thrombocytopenic purpura (ITP) in the absence of bleeding or a very low platelet count.34 In children, ITP is often a temporary condition that resolves without treatment. Current guidelines recommend not treating childhood ITP unless there is bleeding or there are factors felt to increase the risk of bleeding.34 In adults, ITP is usually a chronic disease with a relapsing and remitting course over a patient's lifetime. Many patients are able to maintain low but safe platelet counts without treatment. Current guidelines suggest that a patient with a platelet count of >30 000/μL and no bleeding can usually be safely managed with observation alone.34
All ITP treatments involve a risk of harm. Glucocorticoids increase the risk of infection, can impair glucose metabolism, can cause adrenal suppression. and have many other well recognized side effects. In children, chronic glucocorticoid use has also been implicated in growth impairment.35 Splenectomy necessarily involves risks from general anesthesia and surgery. It is also associated with a small but important risk of life-threatening infection—a risk that may be higher in patients previously treated with rituximab, which may cause impaired responses to vaccines.36 Rituximab, although generally well tolerated, can be associated with infusion reactions and hepatitis B reactivation.37,38 Thrombopoietin (TPO) receptor agonists, because they are new agents, have an incompletely defined safety profile. In addition, new ITP treatments such as rituximab and TPO receptor agonists are very expensive. Cost-effectiveness analyses for TPO receptor agonists in particular suggest that they are likely only cost-effective in the setting of severe ITP refractory to other strategies.39,40 For all of these reasons, it is important that patients with ITP are only treated if the anticipated benefits of treatment outweigh the risks.
ASH's second Choosing Wisely® list includes 4 recommendations focused on nonmalignant hematology and 1 recommendation focused on malignant hematology. A similar distribution was apparent in ASH's first list.2 It is important to reflect on why this pattern may be occurring because it seems unlikely that it reflects a true lack of opportunity for harm reduction or stewardship in the practice of malignant hematology.
In both the first and second ASH Choosing Wisely® campaigns, the Task Force received modestly more recommendations related to benign than to malignant hematology. However, the main point of discrimination appears to be when prospective items are scored by the Task Force. Scoring has consistently resulted in more nonmalignant items in the semifinalist list. Although it is possible that this reflects inherent bias within the Task Force, this seems unlikely because malignant hematologists are well represented there. Scrutiny of the suggestions received related to malignant hematology reveals that some have tended to focus on costly but less harmful forms of testing (such as specific molecular tests), some have been narrow in scope, and some have addressed areas of practice that are rapidly evolving and thus lack a solid evidentiary foundation. Items with these features have tended to score less well due to our method of prioritizing harm avoidance over cost reduction and our emphasis on established evidence and impact.
There are some aspects of malignant practice that have been almost absent from the pool of suggestions submitted to the 2 ASH Choosing Wisely® campaigns. For example, over the course of 2 campaigns, only 3 suggestions have directly related to stem cell transplantation. Given the high risks and the costs of stem cell transplantation, it seems likely that there are tests and/or treatments in this field that could be questioned.
Whether there will be a third ASH Choosing Wisely® Campaign has not yet been determined; if there is, the Task Force may need to consider different methods of engaging the malignant hematology community. In addition, through this article, we on the Task Force challenge the malignant hematology community to reflect on which tests, treatments, and procedures commonly used in malignant hematology we would all benefit from questioning.
In closing, 2 final issues warrant comment. Readers are reminded that the ASH Choosing Wisely® recommendations were developed to encourage conversations between health care professionals and patients. They are not intended to replace clinical judgment, nor are they intended to guide funding decisions. Finally, medicine is dynamic and it is possible that particular Choosing Wisely® recommendations will need to be revised and/or modified as the evidence evolves. The Choosing Wisely® Task Force, under the auspices of the ASH Committee on Quality, is currently developing a protocol to review and revise existing recommendations on a regular basis.
This article was selected by the Blood and Hematology 2014 American Society of Hematology Education Program editors for concurrent submission to Blood and Hematology 2014. It is reprinted with permission from Blood 2014, Volume 124.
Acknowledgments
This work was supported by the American Society of Hematology. Robert Plovnick and Patrick Irelan (ASH staff) provided administrative and organizational assistance to the project. Adam Haynes is a professional methodologist contracted by ASH. The following individuals acted as expert external reviewers for one or more ASH Choosing Wisely® items: John C. Byrd, George R. Buchanan, Doug B. Cines, Mark A. Crowther, Adam Cuker, David A. Garcia, Neil Goldenberg, Craig S. Kitchens, Sophie Lanzkron, Richard Lottenberg, Keith R. McCrae, Stephan Moll, Cindy E. Neunert, Kanti R. Rai, Tait D. Shanafelt, and Theodore E. Warkentin.
Disclosures
Conflict-of-interest disclosures: The authors declare no competing financial interests. Off-label drug use: None disclosed.
Correspondence
Lisa K. Hicks, 30 Bond St., Rm 2-084 Donnelly Wing, Toronto, Ontario M5B 1W8, Canada; Phone: (416) 864-5632; Fax: (416) 865-3055; e-mail: hicksl@smh.ca.
