
Abstract
A majority of patients with acute myeloid leukemia (AML) will relapse after achieving complete remission. At relapse, patients should be risk stratified and a decision made about the appropriateness of intensive therapy and whether a potentially curative allogeneic stem cell transplantation (allo-SCT) is possible. Risk factors include duration of first complete remission and adverse cytogenetics, as well as age and FLT3 mutation status. Available therapies are steadily increasing, but for the most part should be regarded as either best palliation or as a bridge to allo-SCT. Simple symptomatic therapies for patients with extreme age or the worst prognosis should also be considered. Newer therapeutic options include novel cytotoxic chemotherapies including clofarabine, immunomodulatory agents, targeted therapies against FLT3 and mTOR, and immunoconjugates. All patients with relapsed AML should be considered for an appropriate clinical trial.
Introduction
The age-adjusted incidence of acute myeloid leukemia (AML) is 3.6 per 100 000 persons per year,with a median age at diagnosis of 66 years.1 Whereas the outcome for patients with AML who are less than 60 years of age has improved over the past several decades, the major reasons for failure to achieve cure in the majority of these are primary refractoriness of disease to initial chemotherapy or failure to maintain the complete remission that has been achieved (relapse). Indeed, with the exception of a minority of patients with specific subtypes of AML (eg, acute promyelocytic leukemia2 and core-binding factor–positive AML3 ), relapse is associated with an extremely poor prognosis, and this has been the group of patients most actively enrolled into clinical research studies of new agents and approaches. Recent studies have demonstrated that relapse is associated with the acquisitions of identifiable mutations that were not present before therapy.4 Whereas some of these patients have achieved very long remissions with nontransplantation therapies, the only consistently curative therapy for relapsed AML is allo-SCT.
Previous studies have demonstrated that repeated cycles of treatment may be required to optimize outcomes from primary therapy in AML and that greater intensity of therapy is associated with improved outcome.5–7 Therefore, the adequacy of primary therapy is an important factor to be considered in deciding on the subsequent clinical care of these patients, which raises the question of whether the majority of patients who are successfully salvaged by second-line standard chemotherapy for relapsed AML are those who were suboptimally treated in the first line due to assigned protocol, toxicity, complications or other factors.
Patterns of relapse
Relapse of AML after successful induction therapy is most commonly recognized by overt hematologic relapse with the reappearance of circulating blasts and cytopenias, although it may also be identified (particular in the early period after induction when monitoring is more intense) by the reappearance of an informative molecular or cytogenetic marker, or more controversially, an informative flow cytometry pattern. These forms of relapse are generally referred to as minimal residual disease and may reflect a less urgent clinical scenario.8 The reappearance of a previously absent PML-RARα signal in a patient with acute promyelocytic leukemia or a BCR-ABL signal in Philadelphia chromosome–positive AML are the best validated forms of molecular relapses, with particular therapeutic strategies including small molecules targeted at the oncogene.
Prognostic factors and scoring proposals
Importance of duration of CR1 and karyotype
For patients with relapsed disease, it has been recognized for some time that the duration of first complete remission (CR1) heavily influences outcome after salvage therapy for subsequent relapse. MD Anderson Cancer Center data from more than 20 years ago clearly showed a cut point for the likelihood of achieving a second CR (CR2) at a minimum CR1 duration of 12 months,9 whereas other investigators have shown that CR2 rates were extremely poor (< 20%) when CR1 was < 6 months.10 Based on an analysis of outcomes of more than 600 patients with AML in first relapse, investigators from the Netherlands, Belgium, and Switzerland presented the European Prognostic Index (EPI).11 The EPI (subsequently validated in a US-based study12 ) identified 4 independent factors influencing outcome after salvage therapies: increased age, shorter duration of CR1, unfavorable karyotype at initial diagnosis, and prior allo-SCT. The most favorable group had a 46% 5-year overall survival, with the intermediate group at 12% and the poorest-risk group at 6%. The relatively recent demonstration of the adverse impact of FLT3 internal tandem duplications at diagnosis has also been confirmed as an additional factor to be considered when evaluating the prognosis of relapsed patients.13
A new prognostic score was proposed by the Groupe Ouest Est d'Etude des Leucémies et Autres Maladies du Sang (GOELAMS), which incorporated FLT3 mutations but excluded age and prior allo-SCT from the European Prognostic Index (EPI), and has since been validated.14 Again, early relapse from CR1 predominates as a prognostic indicator, along with FLT3 mutations and high-risk cytogenetics at diagnosis.
Table 1 provides a description of the GOELAMS and EPI scores. Interpretation of these scores requires an understanding of the age range of the subjects used to establish the score and the range of therapies offered. Therefore, if a study focuses on a nontransplanted group, outcomes might be quite different because there is no guarantee that the same factors affect outcome after intensive chemotherapy as affect outcome after allo-SCT.
Prognostic scores in relapsed AML
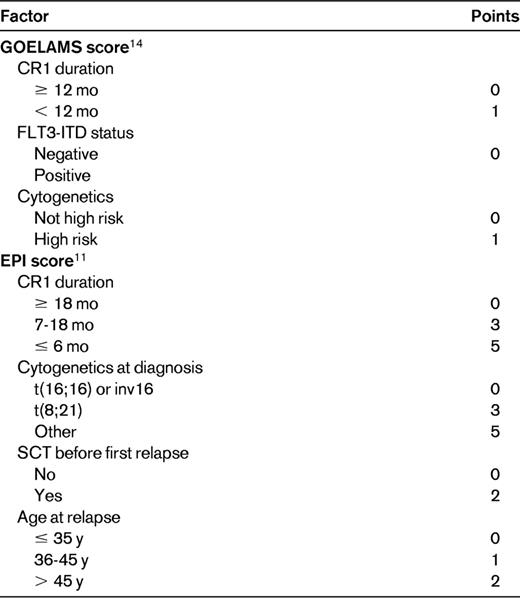
Two-year outcome: 0 points (good): OS 58%, EFS 45%; 1 point (intermediate): OS 37%, EFS 31%; 2 or 3 points (poor): OS 12%, EFS 12%. One-year/5-year outcome: 0-6 points (good) OS 70%/46%; 7-9 points (intermediate) OS 49%/18%; 10-14 points (poor) OS 16%/4%.
FLT3-ITD indicates FLT3 internal tandem duplication.
The problem of relapse after prior allo-SCT for patients with AML in CR1
Whereas it is generally acknowledged that allo-SCT offered in CR1 for patients with intermediate- and high-risk AML offers the best chance of cure, it is also recognized to be a high-risk treatment with a failure rate that also includes relapse.15 Whereas achieving CR2 may be a target in these patients, decisions regarding the use of immunotherapy in the form of withdrawal of immunosuppression, addition of donor lymphocyte infusion, or second transplantations are dependent on the type of donor used, the availability of second donations, and GVHD status of the patient at the time of relapse. Again, the interval between first transplantation and relapse is demonstrably important in making therapeutic decisions.16 This is clearly a situation where individualization of therapeutic decisions is appropriate. Patients who have a low volume of disease burden and can be induced into CR2 or have relapsed late after first hematopoietic SCT are most likely to do better whatever the choice of subsequent therapy.
Aims of salvage treatment
Whereas many treatment approaches have been studied in recent years, it is clear that long-term disease-free survival and possible cure is still only a realistic aim with allo-SCT, with the possible exceptions of acute promyelocytic leukemia and patients who were inadequately treated with primary therapy. Therefore, all therapies for relapse should be offered with the aim of proceeding to some form of allo-SCT for which the achievement of CR2 either before or after allo-SCT is the goal.17 When allo-SCT is not possible or available, the role of salvage treatment should be considered as the best available palliative therapy, and may take the form of intensive combination chemotherapy, experimental therapy, low-dose single-agent therapy (eg, cytarabine given by intermittent subcutaneous injection, oral hydroxyurea, or 6-thioguanine) or symptomatic therapy only with transfusions of needed blood products, analgesics, and so on.18 Table 2 provides examples of salvage regimens.

New approaches to treatment of relapse
Many chemotherapeutic agents other than the standard anthracyclines and cytarabine have been reported as having activity in relapsed AML. When the intent is to prepare a patient for allo-SCT, efficacy and toxicity are both important considerations. In many centers in which a nucleoside analog is not used in primary therapy, fludarabine (used as a potentiator of arabinofuranosylcytosine triphosphate incorporation) is often used as salvage therapy in combination with cytarabine, sometimes with recombinant human granulocyte colony stimulating factor, the so-called FLAG regimen, which has a demonstrable CR rate.19 Activity has general been modest, although CRs were reported in refractory patients in nonrandomized studies. Results from a randomized study have not shown a demonstrable benefit using this regimen.20 Current studies involving newer nucleoside analogs and a variety of other agents are ongoing. Some of the more promising agents are described below.
Clofarabine
Clofarabine, a novel purine analog, has been mostly studied in pediatric acute lymphoblastic leukemia, but has also been evaluated either as a single agent or in combination with cytarabine in several early-phase studies in relapsed AML21,22 and in the primary therapy of elderly patients.23 There was a demonstrable response rate, but it was modest and variable. Up to 42% of adults with relapsed or refractory AML who were shown to have a CR either used clofarabine as a single agent or in combination with cytarabine, although one of the studies produced only a single CR of 15 patients despite identical dosing. The major toxicities of clofarabine have been hepatic, gastrointestinal, and cutaneous.
Tosedostat
Tosedostat, an orally available aminopeptidase inhibitor, has intriguing chemical properties that result in the active metabolite accumulating intracellularly. A recent phase 1/2 study with this agent in relapsed AML and myelodysplastic syndrome (MDS) demonstrated significant clinical activity, with an overall response rate of 27%.24 This agent is therefore of interest for further study in this patient group.
FLT3 inhibitors
Several small-molecule inhibitors have been and continue to be studied in relapsed AML in this very-high-risk group of patients. These agents include lestaurtinib, midostaurin, sorafenib, and quizartinib (AC220), and the results have generally shown minimal to modest activity.25–27 None of these agents is capable of inducing CR2 with any reliability and if they are to be used in therapy combinations with other agents, a detailed understanding of specific mutations will be required. A recent report with AC220 showed a relatively high CR rate (45%), but specific mutations conferring AC220 resistance emerged in the majority of patients, resulting in relapse.28 This promising agent may have a role as a bridge to transplantation for these difficult patients, and at least one international study is addressing this very issue (www.clinicaltrials.gov identifier NCT00989261).
mTOR inhibitors
Inhibitors of the mammalian target of rapamycin (mTOR), such as sirolimus and everolimus, which are more commonly used in solid organ transplantation as immunosuppressive agents, are potentially targeted for therapy in relapsed AML given the role of the mTOR pathway in cytarabine activity.29 Studies are under way by many groups after early demonstrations of clinical activity of these agents.30,31
Hypomethylating agents
Decitabine and 5-azacitidine are hypomethylating agents active in a significant number of patients with MDS. The studies that confirmed their activity permitted patients with 20%-29% BM blasts defined as MDS in the French-American-British classification but AML in the current World Health Organization system. It is clear that some of these patients with AML can benefit from exposure to these agents. The sometimes months-long time to response in MDS precludes an expectation of success in highly proliferative AML, and there are data to support the use of 5-azacitidine in more indolent disease, particularly in the elderly.32 Overall, as a single agent, responses, when seen, are of short duration. In salvage therapy of AML, this group of drugs is likely to be useful in low volume or early relapse or in combination with other agents. 5-azacitidine is currently under study as maintenance therapy after allo-SCT.33
Immunomodulatory agents
Histone deacetylase inhibitors
Agents such as vorinostat have been shown to have some limited activity in advanced AML. A recent phase 2 study of vorinostat in combination with cytarabine and idarubicin demonstrated tolerability and an overall response rate of 85% in newly diagnosed patients.36 Further study in combination with standard agents are warranted in relapsed AML as well.
Gemtuzumab ozogamicin
Gemtuzumab ozogamicin, a calicheamicin immunoconjugate, has had a difficult development path despite having shown significant single-agent activity in CD33+ AML and being incorporated into several clinical trials of AML, including the large United KingdomMedical Research Council study AML15.37 Excessive toxicity, in particular, hepatotoxicity, resulted in its withdrawal from the United States and many other markets in 2011; however, a study presented at the 2011 ASH annual meeting suggested that it may well have a role in AML management, particularly as a bridge to transplantation.38
Allo-SCT
As indicated previously, allo-SCT has an established track record in the cure of relapsed and refractory AML, although even in this situation, subsequent relapse is the major reason for failure. The earliest studies with allo-SCT were in the refractory group of patients, in whom a cure rate of approximately 10% was identified, a figure that has not been improved upon significantly.
In relapsed AML, the questions raised around transplantation include when to perform the transplantation, what type of transplantation (eg, conditioning intensity and source of stem cells) should be used, and whether to use chemotherapy to attempt CR2 before transplantation.
Early studies suggested that immediate transplantation at identification of relapse produced optimal results. The era was one of matched sibling donors and myeloablative conditioning regimens,39 and this combination would now be used in a minority of transplantation recipients. In the modern era, despite demonstrably improving outcomes,40 suitable unrelated donors can take months to identify and are only identified for a minority of suitable patients.41 Cord blood units can be identified more rapidly, but are limited by expense and access to rooms at the hospital for adults due to prolonged lengths of inpatient stay resulting from delayed engraftment,42 and because haploidentical transplantations are still at an early stage of clinical development (reviewed by Ballen et al43 ). In addition, the use of reduced intensity or nonmyeloablative conditioning regimens, which are currently favored for the majority of patients with AML due to reduced acute toxicity, has a prolonged time to development of a GVL effect and is therefore inappropriate for patients with high-volume or proliferative AML.44
Most patients with relapsed AML will require some form of disease control before allo-SCT to achieve a state of CR2 or MRD. The timing and type of transplantation will be heavily dependent on the clinical status of the patient, the availability of a stem cell source, and locally available resources.
A personal approach to the management of relapsed AML is described in Figure 1, with acute promyelocytic leukemia being described separately due to its special characteristics and better prognosis with non–allo-SCT therapy.

How I treat relapsed AML. AML indicates acute myeloid leukemia; and APL, acute promyelocytic leukemia.
How I treat relapsed AML. AML indicates acute myeloid leukemia; and APL, acute promyelocytic leukemia.
Conclusion
Relapsed AML remains a significant clinical challenge and, as therapeutic options increase, it is likely that the burden of relapse will also increase. Treating clinicians require vigilance in the early identification of patients at high risk of relapse and the selection of therapeutic options if this should occur, including early identification of a source of allogeneic stem cells, ideally in collaboration with an experienced transplantation center.
This decision-making process must take into account the suitability for an individual patient and particular thought must be given to the appropriateness of available therapies, particularly for the elderly and those with the highest risk scores. Given the overall poor prognosis of relapsed AML, clinical trial participation should be considered for all such patients.
Disclosure
Conflict-of-interest disclosure: The author is on the board of directors, advisory committees, or speakers bureaus of Celgene, Novartis, Pfizer, and Alexion; serves as a consultant for Pfizer and Alexion; and receives honoraria from Alexion. Off-label drug use: Lenalidomide (relapse of AML); Rapamycin (relapse of AML); 5-azacitidine (maintenance therapy after allo-SCT).
Correspondence
Jeffrey Szer, Department of Clinical Haematology and BMT Service, 2 Centre, The Royal Melbourne Hospital, Parkville, VIC 3050, Australia; Phone: +61-3-9342-7737; Fax: +61-3-9342-7386; e-mail: jeff.szer@mh.org.au.
