
Abstract
Advances in hematopoietic stem cell transplantation (HSCT) and immunosuppressive therapy (IST) have improved survival in severe aplastic anemia (SAA) from 10%-20% in the 1960s to 80%-90% today. A matched sibling HSCT is the treatment of choice in younger patients, whereas IST is often used in older patients or in those who lack a histocompatible sibling. Graft rejection, GVHD, and poor immune reconstitution (with associated infectious complications) limit the success of HSCT, whereas lack of response, relapse, and clonal evolution limit the success of IST. The historically high rate of graft rejection in SAA is now less problematic in the matched setting, but with greater rates observed with unrelated and umbilical cord donors. The correlation of increasing age with the risk of GVHD and the significant morbidity and mortality of this transplantation complication continue to affect the decision to pursue HSCT versus IST as initial therapy in adults with SAA. Outcomes with matched unrelated donor HSCT have improved, likely due to better donor selection, supportive care, and improved transplantation protocols. Results with mismatched unrelated donor and umbilical HSCT are not as favorable, with higher rates of graft rejection, GVHD, and infectious complications. Investigation of several upfront alternative IST protocols has not improved outcomes beyond horse antithymocyte globulin and cyclosporine. More recently, the role of alemtuzumab in SAA has been better defined and an oral thrombomimetic, eltrombopag, is showing promising activity in refractory cases. The most recent advances in HSCT and IST in SAA are discussed in this review.
Introduction
Severe aplastic anemia (SAA) is almost always fatal if untreated. Mortality ensues from complications of pancytopenia, a hallmark in AA. Five decades ago, there was little to offer patients with SAA, with androgen therapy and transfusion support often used at that time. Unfortunately, most patients died 1-2 years after diagnosis from infections and/or hemorrhagic complications. Much has evolved since the 1960s in the management of SAA, and most patients (> 85%-90%) today are expected to be alive in the years after the diagnosis.1 The principal interventions responsible for these improved outcomes are hematopoietic stem cell transplantation (HSCT) and immunosuppressive therapy (IST).
AA is usually diagnosed in the setting of pancytopenia and a hypocellular BM when other diseases such as myelodysplasia, myelofibrosis, and certain leukemias are excluded. SAA is diagnosed when 2 of 3 blood counts are met: absolute neutrophil count < 500/μL, absolute reticulocyte count < 60 000/μL, and platelet count < 20 000/μL.2 Occasionally, AA is diagnosed serendipitously when a routine hemogram is done as part of a check-up or during blood donation or preoperative evaluation. In these cases, the pancytopenia is often nonsevere, but can worsen over time into the severe range. Once a diagnosis of SAA is established, therapy should not be delayed in the hope of spontaneous recovery, because this approach is unlikely to be fruitful and will inevitably delay therapy with HSCT or IST. On occasion, withholding a drug strongly suspected to be associated with pancytopenia and BM hypocellularity (eg, certain antibiotics and chemotherapeutic agents) is reasonable for a few weeks. However, a prolonged delay before initiating primary treatment is not advisable and can result in serious complications before definitive therapy.
Large prospective studies have defined the limitations of IST and HSCT in SAA. Hematologic response can be achieved in 60%-75% of patients, with younger patients experiencing a higher response rate.3,4 Among responders, relapse is observed in approximately 30%-40%, with the majority responding to more immunosuppression.5,6 More problematic is clonal evolution to myelodysplasia, which is diagnosed when a new cytogenetic abnormality or characteristic dysplastic findings in the BM (eg, increases in blasts or micromegakaryocytes) are identified in follow-up. The most common cytogenetic abnormality is monosomy 7, which associates with worsening blood counts, refractoriness to immunosuppression, and progression to high-grade myelodysplasia and leukemia.7 Other cytogenetic findings can appear over time (eg, del13q, trisomy 8, and del20q), which may or may not be associated with progression to myelodysplasia. These other karyotypes can be transient and not associated with dysplastic findings in the BM or worsening blood counts, being at times of uncertain clinical significance. In general, with sustained engraftment, HSCT precludes the late complications of relapse and clonal evolution observed with IST. However, graft rejection (which is more frequent now with alternative donors), acute and chronic GVHD, and infectious complications can occur. Therefore, despite similar outcomes with either treatment modality, distinct short- and long-term complications limit the success of these therapies in the clinical setting.
Initial therapy for SAA
HSCT
After diagnosing a patient with SAA, the first decision the hematologist confronts relates to the initial treatment modality. In practice, the factors that will guide in the decision-making process include age, presence of a histocompatible donor, and comorbidities. In children and young adults with a matched sibling donor (MSD), a related HSCT is the initial treatment of choice, and in older patients, IST is often used. All younger patients without an MSD should be screened at the time of initiating IST for potential histocompatible donors in BM registries.
In a recent large retrospective study including 1300 SAA patients from the Center for International Blood and Marrow Transplant Research (CIBMTR), survival was inversely correlated with age.8 At 5 years, 82% of those under 20 years of age were alive compared with approximately 50% for those over 40.8 An increased rate of GVHD more frequently complicated transplantation outcomes in older patients compared with children and young adults. In a retrospective analysis from the Seattle group of 23 patients over the age of 40, MSD HSCT as first therapy resulted in survival of 65%, similar to the CIBMTR data.9 The upper age limit we use is 40 years, because the risk of GVHD and transplantation-related mortality increases after this age.8,10,11 At any age, the presence of significant comorbidities should favor IST as the initial treatment modality of choice. Our general approach in the initial management of SAA is depicted in Figure 1.

Algorithm for initial management of SAA. In patients who are not candidates for a matched related HSCT, immunosuppression with horse ATG + CsA should be the initial therapy. We assess for response at 3 and 6 months, but usually wait 6 months before deciding on further interventions in nonresponders. In patients who are doing poorly clinically, with persistent neutrophil count < 200/μL, we proceed to salvage therapies earlier, between 3 and 6 months. Transplantation options are reassessed at 6 months and donor availability, age, comorbidities, and neutrophil count become important considerations. We favor a matched UD HSCT in younger patients with a histocompatible donor and repeat IST for all other patients. In patients with a persistently low neutrophil count in the very severe range, we may consider a matched UD HSCT in older patients. In patients who remain refractory after 2 cycles of IST, further management is then individualized by taking into consideration suitability for a higher-risk HSCT (ie, mismatched UD, haploidentical or UC donor), age, comorbidities, neutrophil count, and overall clinical status. Some authorities in SAA consider 50 years of age as the cutoff for sibling HSCT as frontline therapy. Adapted with permission from Scheinberg and Young.1
Algorithm for initial management of SAA. In patients who are not candidates for a matched related HSCT, immunosuppression with horse ATG + CsA should be the initial therapy. We assess for response at 3 and 6 months, but usually wait 6 months before deciding on further interventions in nonresponders. In patients who are doing poorly clinically, with persistent neutrophil count < 200/μL, we proceed to salvage therapies earlier, between 3 and 6 months. Transplantation options are reassessed at 6 months and donor availability, age, comorbidities, and neutrophil count become important considerations. We favor a matched UD HSCT in younger patients with a histocompatible donor and repeat IST for all other patients. In patients with a persistently low neutrophil count in the very severe range, we may consider a matched UD HSCT in older patients. In patients who remain refractory after 2 cycles of IST, further management is then individualized by taking into consideration suitability for a higher-risk HSCT (ie, mismatched UD, haploidentical or UC donor), age, comorbidities, neutrophil count, and overall clinical status. Some authorities in SAA consider 50 years of age as the cutoff for sibling HSCT as frontline therapy. Adapted with permission from Scheinberg and Young.1
Until 10-15 years ago, BM was the sole source of stem cells for HSCT. Since the late 1990s, peripheral blood stem cells (PBSCs) derived from G-CSF mobilization gained in popularity as a less-invasive outpatient procedure and with a greater CD34+ yield. However, several groups have now reported worse outcomes with G-CSF–mobilized PBSCs compared with BM-derived CD34+ cells in SAA.12–15 Initially, this observation was made in a retrospective analysis from Europe, in which 27% of those under 20 years of age experienced chronic GVHD, compared with 12% in the same age group.12 In a separate analysis in the United States, the rate of GVHD was also higher with PBSCs compared with BM grafts in patients of all ages, and this observation was also extended recently to unrelated donor (UD) HSCT.13,14 Because there is no benefit from GVHD in a nonmalignant disorder such as AA, BM should be the preferred source of stem cells outside of a clinical research protocol.
Several transplantation protocols have been used in SAA over the years, but a popular regimen includes cyclophosphamide (Cy) + antithymocyte globulin (ATG) as conditioning and cyclosporine (CsA) + methotrexate as GVHD prophylaxis.3 The combination of Cy/ATG was not superior to Cy alone in a randomized study16 ; nevertheless, Cy/ATG–based conditioning remains widely used in HSCT protocols for SAA. The addition of fludarabine (Flu) to Cy/ATG has been shown to overcome the risk of rejection in heavily transfused or older patients undergoing MSD HSCT and may be an option in these settings.11,17 Another potent lymphocytotoxic immunosuppressant, alemtuzumab (Alem), has been investigated in place of ATG in transplantation protocols. In a recent retrospective analysis from the United Kingdom of 50 patients (21 MSD and 29 UD HSCT), Flu/Cy + Alem yielded a rejection rate of 9.5% in MSD transplantations and low rates of acute (17%) and chronic GVHD (7%) at 1 year.18 There were 2 cases of posttransplantation lymphoproliferative disease (with 1 death), 9 cases of CMV reactivation (1 CMV disease), and 7 cases with adenovirus viremia. As expected, mixed T-cell chimerism was frequent, with a median of 45% CD3 chimerism at 100 days.18 In this retrospective study, the low rate of GVHD with PBSC grafts (n = 14) is of potential interest, because an Alem-based conditioning may reduce the negative impact in GVHD associated with this source of stem cells. This will need to be confirmed in larger prospective studies.
IST
The efficacy of IST in SAA is well established, with several large prospective trials in the United States, Europe, and Japan showing consistent results.3 The standard IST regimen is with horse ATG + CsA, which produces hematologic responses in 60%-75% of cases.3 Children do better with horse ATG/CsA, with response rates of 75% reported in different studies,4,19,20 whereas older patients tend to have a lower response rate that approximates 50%.21,22 The strongest predictor for long-term survival after IST is hematologic response, with a robust recovery associated with the best long-term survival outcomes.2 It is important to note that the survival benefit applies to all responders to IST, either partial or complete. At our institution, we define hematologic response when criteria for SAA is no longer met at 6 months, which almost always equates to achieving transfusion independence.2
The greatest experience in SAA is with horse ATG, which is the preparation most widely studied in large prospective trials.1,3,22,23 In the past 10-15 years, a different ATG formulation from rabbits has gained in popularity in SAA. Initially, rabbit ATG was used in the refractory and relapsed settings and showed good activity as a salvage regimen.5,24 The greater lymphocytotoxicity of rabbit ATG was also shown to be superior in protecting kidney allografts compared with horse ATG.25 These data led to the perception that rabbit ATG might be superior to horse ATG as frontline therapy in SAA.
The results from retrospective studies comparing historical outcomes between the 2 ATGs as first therapy have been mixed, with the majority of studies showing superiority of horse over rabbit ATG and a few studies showing no difference (Table 1).1 A large prospective, randomized study at the National Institutes of Health (NIH) addressed this question more definitively. This study, conducted over 6 years, randomized 120 patients to either horse (n = 60) or rabbit (n = 60) ATG. At 6 months, the rate of hematologic response was markedly inferior with rabbit ATG (37%) compared with horse ATG (68%), an unanticipated outcome. This study was originally designed and powered to show the opposite, that rabbit ATG would be superior to horse ATG. The difference in response rate resulted in a significant survival difference, with 70% of patients alive at 3 years after rabbit ATG compared with 94% with horse ATG.23 Therefore, the results from this randomized trial support the continued use of horse ATG over rabbit ATG as first therapy for SAA.
Studies comparing horse and rabbit ATG/CsA as first therapy in SAA
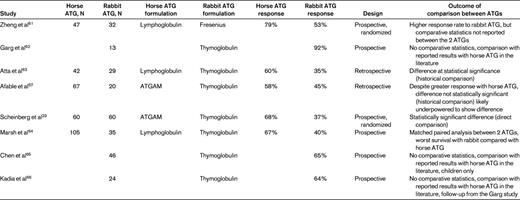
Only published manuscripts are depicted in the table. Other studies comparing horse and rabbit ATG as first therapy have been reported in abstract form only. For consistency, hematologic response rates at 6 months are shown whenever possible. Recent uncontrolled reports from Asia (mostly in abstract form) using rabbit ATG are showing results superior to that observed in the United States and Europe as frontline therapy in SAA, suggesting an influence of ethnicity in outcomes after rabbit ATG. Adapted with permission from Scheinberg and Young.1
The addition of other immunosuppressants (eg, mycophenolate mofetil or sirolimus) or growth factors to standard horse ATG have not improved the outcomes of IST.22,26,27 A large randomized study comparing outcomes of horse ATG/CsA with or without G-CSF did not show a difference in the rates of hematologic response, event-free or overall survival.22 This result confirmed prior studies exploring G-CSF in addition to immunosuppression in SAA. Therefore, our practice has been not to include routine G-CSF with IST protocols, but may consider its use in selected cases.
In general, our approach has been to wait 6 months after ATG to determine responsiveness to the initial course. The majority of responses to horse ATG do occur by 3 months, with 5%-10% of responders improving between 3 and 6 months. Hematologic responses after 6 months are very infrequent, and our practice is to consider alternative therapies at this time point. In cases in which continued support cannot be envisioned for 6 months due to deteriorating blood count and clinical conditions, we tend to proceed to alternative salvage therapies earlier between 3 and 6 months.
Salvage therapies for SAA
Despite great advance brought by the use of ATG in SAA, approximately 1/3 are expected not to respond and 1/3 of responders anticipated relapsing after initial therapy with horse ATG.3 The approach in each of these scenarios will again depend on age, availability of a histocompatible donor, and comorbidities. The absolute neutrophil count may also influence in the decision-making process regarding choice of therapy in these settings (Figure 1).
Refractory SAA
In older patients with MSD who remain severely pancytopenic at 6 months after horse ATG, a related HSCT should be considered in the absence of significant comorbidities. An active infection in general precludes HSCT, but we have proceeded with transplantation if the infection is controlled with antimicrobials, because most serious infections (in particular fungal) are not likely to resolve in the setting of persistent severe neutropenia.
In younger patients with a histocompatible UD, HSCT should be considered. Results from matched UD HSCT have improved in recent years, with some reports in children suggesting that transplantation outcomes in this age group rivals that of an MSD HSCT.28–30 However, these results are not consistent with other large cohorts suggesting that outcomes may not be as favorable as those of MSD HSCT.31–34 Conditioning in the UD setting has been varied and the optimal regimen not yet defined (Table 2).1 Long-term outcomes of children who received radiation-free conditioning for MSD HSCT did not reveal growth or developmental impairments after decades.35 Therefore, avoidance of radiation remains a goal in UD HSCT protocols; however, these regimens have been associated thus far with an increased risk of rejection.33,36 More recently, Flu/Cy/Alem was associated with a graft failure rate of 15% in UD HSCT and with low rates of acute and chronic GVHD, and may emerge as an alternative radiation-free regimen in UD HSCT.18 Nevertheless, many transplantation protocols still include low-dose total body irradiation in the conditioning before UD HSCT to improve graft acceptance and, hopefully, to reduce the long-term risks associated with radiation exposure at a young age (Table 2).1
Studies of UD HSCT in SAA
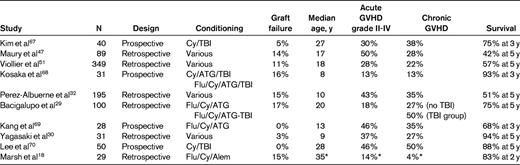
Outcomes shown are for the entire cohort reported in each study. Studies that include 4 or more conditioning regimens are reported as “various.” Only studies with greater than 20 patients reported in the past 5 years are depicted. For Viollier et al,51 only the most recent cohort (after 1998) reported is shown. The Marsh study reported on outcomes in 50 patients total, 21 of whom received an MSD HSCT and 29 a UD HSCT after Flu/Cy/Alem conditioning. The reported median age and rates of acute and chronic GVHD are for the entire cohort (all 50 patients). All acute GVHD cases in the Marsh study were grade I-II. Adapted with permission from Scheinberg and Young.1
TBI indicates total body irradiation.
In patients who lack a histocompatible donor, we prefer to proceed with a second course of IST over a high-risk transplantation from a mismatched unrelated, haploidentical, or umbilical cord (UC) donor, where the risks of graft rejection, transplantation related mortality, infectious complications and GVHD are higher than that of matched related or UD HSCT.31,32,37–39 The greater experience in refractory SAA is with rabbit ATG, for which reported responses have ranged from 30%-77%.5,24 More recently, a similar experience was reported with the anti-CD52 mAb Alem. Fifty-four patients who failed initial horse ATG were randomized to rabbit ATG (n = 27) or Alem (n = 27): hematologic responses were observed in 30%-40% of patients at 6 months with either agent.40 Alem was well tolerated and associated with fewer infusion related toxicities compared with rabbit ATG. This response rate of 30%-40% has been steady at our institution for the past 10 years, with repeat IST in horse ATG failures.5,40 Survival at 3 years was 83% for Alem- and 60% for rabbit ATG–treated patients.40 CsA was not administered in the Alem arm, which avoided many of the side effects associated with this agent, particularly in older patients and in those who experienced poor tolerability to CsA. Smaller pilot studies using Alem with CsA have shown feasibility of this combination for SAA.41–43 Therefore, the role of CsA added to an Alem-based regimen is not yet defined.
Relapsed SAA
The response rate to repeat IST in the relapsed setting is approximately twice that observed in refractory patients.1 Most of the recent experience in relapsed SAA is again with rabbit ATG/CsA, with response rates observed in 60%-70% of cases.5 Alem has also has been investigated in this setting in 25 patients in a single-arm study. The response rate to this single agent was 56% at 6 months and the survival at 3 years was 86%.40 As in the refractory patients, CsA was not administered with the Alem regimen.
With a higher hematologic response rate to IST in relapsed patients, our approach in general is not to recommend a UD or MSD HSCT in older patients in first relapse. Reintroduction or an increase in CsA dose for 2-3 months can be effective, with a repeat course of IST used in those unresponsive to the outpatient CsA regimen. Preventing relapse altogether after h-ATG/CsA is important and a few strategies have been adopted toward this goal. A common practice is to prolong full-dose CsA use beyond 6 months (usually for 12 months) and implement a slow taper afterward. Although logical, few studies have looked at this approach systematically. In a retrospective Italian study, records from 42 pediatric patients treated from 1991 and 1999 were reviewed.44 The CsA taper regimen varied between patients, but 3 groups were retrospectively defined in this study. The cumulative incidence of relapse was 7.6% in the “slower” CsA taper group, compared with 60% in the “rapid” taper group. More recently, a large NIH experience on CsA taper was presented. In this study, all consecutive patients who received a horse ATG–based regimen from 2003-2010 (n = 102) had the CsA dose tapered prospectively (25% every 3 months) after 6 months once hematologic response was achieved (in 67 patients). At 3 years, the cumulative incidence of relapse was 29%, which did not differ from the large historical relapse rate of 32% in patients treated before 2003 when CsA was discontinued at 6 months.45
When improvement in blood counts is achieved in relapsed patients, our practice has been to continue CsA for at least 6-12 months, followed by a very gradual taper as tolerated. In some cases, the CsA can be tapered off completely, but in others, a gradual decline in blood counts can occur with the taper. These patients are likely to require CsA to prevent worsening of pancytopenia and it is our practice to target the lowest CsA dose to maintain adequate blood counts. In most cases, the dose that achieves this goal is in a range in which patients do not experience CsA-related toxicities. On occasion, this may represent a very low CsA dose (such as 25 mg/d), which the patient may not tolerate, being discontinued due to a fall in counts. The management of relapsed patients who respond to IST has not been studied systematically, and other practices may differ from our approach. When a hematologic response is not achieved with IST and severe pancytopenia persists, our general approach has been to pursue transplantation options as outlined in the refractory SAA session.
Evolving concepts in SAA
HSCT
Although most treatment algorithms include patients up to the age of 40 years for HSCT as frontline therapy, some propose extending the cutoff age to 50 in view of favorable outcomes with reduced-intensity MSD HSCT in the 40-50–year age group.9,18,46 Across many studies, increased age is correlated with greater transplantation-related complications and worse survival.8,10,11 Therefore, the decision to pursue MSD HSCT in this age group may need to be individualized by taking into account comorbidities, transplantation center experience, history of complications associated with pancytopenia, access to transplantation, and patient preference.
With the better outcomes of MUD HSCT in younger patients, some have proposed that this modality be offered as initial therapy in SAA. The factors contributing to the better outcome are likely a more stringent donor selection with high-resolution tissue typing and better transplantation protocols with superior antimicrobial and transfusional supportive care.47,48 However, one of the principal difficulties in determining efficacy with this treatment modality is the retrospective nature of most studies, with their large variability in patient selection, transplantation regimens, and reported outcomes. For example, in a recent systematic review of UD HSCT in SAA, reporting variability between studies was such that it precluded a pooled analysis.49 We do not pursue UD HSCT as initial therapy in younger patients for the following reasons: (1) hematologic response to horse ATG in children is high (75%) and long-term survival among responders is excellent, at approximately 90%4,19,20 ; (2) an optimal conditioning regimen is not yet defined; (3) chronic immunosuppression for GVHD is associated with increased morbidity and mortality long-term35,50 ; (4) graft rejection and GVHD remain problematic, especially in older patients; (5) long-term effects of low-dose irradiation (as used in many UD HSCT protocols) is not yet defined; and (6) more generalizable long-term data from larger cohorts are not as favorable as those observed with MSD HSCT.31–33,51 Nevertheless, in practice, these considerations may be moot: practically, the identification of a histocompatible UD and coordination among donor, BM registries, and transplantation centers takes months, and delaying definitive IST during this time may be dangerous. The greater stringency for histocompatibility has limited the available donor pool, and donor identification for non-Caucasians and for those of diverse ethnic backgrounds remains problematic. Therefore, our approach has been to initiate a donor search in all younger patients and to pursue matched UD HSCT upon donor availability should immunosuppression be ineffective, usually at 3-6 months after IST. In this refractory setting, matched UD HSCT has been associated with excellent outcomes in recent years.18,29,52 With this approach, we reserve the risks associated with a UD HSCT to those younger patients not likely to benefit from IST.
Because a histocompatible UD is not available to many patients, alternative stem cell sources have been an area of intense investigation. However, higher rates of GVHD are observed with a mismatched UD HSCT,31,32 and graft rejection, poor immune reconstitution, and susceptibility to viral reactivations remain problematic with UC blood HSCT in SAA.37,38 Transfusion burden does not seem to be a determinant for the greater rejection rate in UC HSCT. In a recent report of 18 patients who received UC HSCT as first therapy, none experienced sustained engraftment.39 Surprisingly, of the 16 evaluable patients (2 early deaths), all had autologous hematologic recovery after conditioning with Flu/Cy/rabbit ATG, resulting in an 89% overall survival at 2 years. Most recent reports using haploidentical donors in HSCT for SAA include a single case or only a few cases. Efforts to make this donor source feasible are exploring methods to manipulate the graft ex vivo or in vivo to reduce rates of GVHD while maintaining adequate engraftment and immune reconstitution.53–55 More promising is the combination of haploidentical and UC blood cells. Preliminary data in 8 patients from the NIH combining haploidentical and UC donor cell grafts after Flu/Cy/horse ATG conditioning is showing promising engraftment of the cord unit (7 of 8 patients) and low rates of GVHD.56 Further accrual and longer follow-up should better define the safety and role of this treatment modality in SAA.
Risk stratification
The ability to identify patients with a higher probability of hematologic response, relapse, clonal evolution, and early mortality (first 1-2 months) may better risk stratify patients and allow for a more logical treatment allocation. In general, very severe neutropenia is associated with greater mortality and higher-risk procedures may be more justified in this group.10,48 Measurement of telomere length and blood counts offers the possibility of rational risk stratification for treatment in future protocols.21,57,58 In a recent report, pretreatment telomere length correlated with relapse, clonal evolution, and survival.58 Patients with shorter telomeres in peripheral blood leukocytes were approximately twice as likely to relapse and 4- to 6-fold more likely to evolve to myelodysplasia or leukemia, with a negative impact on survival.58 If confirmed in other series, this assay might also be useful in determining the level of risk and the need for monitoring of patients after IST.
A minority of patients presenting with “acquired” AA will have a very short telomere length (below the first percentile) and/or carry a mutation in telomerase genes (ie, TERC or TERT).59 A family history of BM failure, idiopathic pulmonary fibrosis, or cirrhosis are clues to the existence of an underlying telomeropathy.59 These findings are associated with dyskeratosis congenita, an inherited form of AA in which children present early in life with pancytopenia and typical physical features including abnormal nails, leukoplakia, and cutaneous eruptions. However, penetrance of telomeropathies is highly variable, and heterozygosity for TERT or TERC mutations can present in older adults in whom the family history can be negative or obscure and who lack pathognomonic physical findings. The best characterization of these patients is not yet certain. We do not label such patients as dyskeratosis congenita (the most severe type linked to DKC1 mutations), but rather as telomere disease or telomeropathy, because the penetrance of the TERT and TERC gene mutations is much lower and the long-term clinical outcomes are currently less clear. Current clinical research protocols at NIH are investigating the impact of telomere length and mutational status on AA outcomes and the effects of androgens on modulating telomere attrition and hematopoiesis in patients with telomeropathies.
Nontransplantation modalities
The emphasis of most IST trials in SAA have been in adding immunosuppressants (eg, mycophenolate mofetil or sirolimus), growth factors (eg, G-CSF), or androgens to the horse ATG/CsA backbone or introducing more potent lymphocytotoxic agents (eg, rabbit ATG or Alem) upfront.1,23,40 Unfortunately, the results of all these efforts have been disappointing, with no significant impact on the outcomes of response, relapse, or clonal evolution beyond what would be expected with horse ATG/CsA alone. Survival, however, has improved over the years, especially among nonresponders, who can now be better supported during periods of severe neutropenia and more successfully undergo salvage therapies with repeat IST or HSCT.48
More recently, an oral thrombomimetic, eltrombopag, has produced hematologic responses in 11 of 25 IST-refractory SAA patients.60 This outpatient regimen was very well tolerated and may become an attractive alternative to patients with persistent pancytopenia after IST. Of interest was the improvement in hemoglobin and neutrophil levels in some of the responders. The improvement in nonmegakaryocytic lineage was surprising and may indicate a stimulatory effect of less committed progenitors. Follow-up studies adding eltrombopag to h-ATG/CsA upfront are currently under way.
Conclusions
The diagnosis of SAA no longer carries the dire prognosis that it did 4 decades ago. In patients who are not candidates for a MSD HSCT, IST with horse ATG/CsA should be the preferred therapy. Outcomes with matched UD HSCT have improved in recent years, so this is becoming the preferred salvage therapy in younger patients who are unresponsive to initial IST. When a histocompatible UD is not available, a second course of IST should be offered before higher-risk transplantation protocols from mismatched unrelated, haploidentical, or UC donors. In the coming years, biomarkers (eg, telomere length, mutational status, and blood counts) or other pathophysiological indicators will likely emerge from global assessments of the immune response and more sensitive measurements of stem cell reserve and function and should provide better guidance in treatment decision in SAA.
Disclosures
Conflict-of-interest disclosure: The author declares no competing financial interests. Off-label drug use: Alem, rabbit antithymocyte globulin, and eltrombopag for AA.
Correspondence
Phillip Scheinberg, Hospital São Jose, Beneficência Portuguesa, Rua Martiniano de Carvalho, 951, São Paulo, Brazil 01321-001; Phone: 55-11-3505-6615; Fax: 55-11-3505-6614; e-mail: scheinbp@mail.nih.gov or phillip.scheinberg@hospitalsjose.org.br.
