
Abstract
Anemia is common in cancer patients. Its cause is multifactorial, so a brief workup is always necessary to rule out simple, reversible causes. Anemia of chronic disease/inflammation and chemotherapy-induced anemia are the most common causes. Symptomatic or clinically severe anemia may require treatment with blood transfusion or an erythropoiesis-stimulating agent (ESA). If ESA therapy is chosen, developing evidence now suggests that, similar to chronic renal failure patients on hemodialysis, the addition of intravenous iron can improve the response to ESA because of iron-restricted erythropoiesis, even in the iron-replete patient.
Introduction
This section discusses the impact of intravenous (IV) iron on anemic cancer patients receiving chemotherapy who are being treated with an erythropoietic-stimulating agent (ESA), beginning with a discussion of why the cancer patient is anemic in the first place. Cancer patients are anemic for one or more of the following reasons, which are listed in Table 1.
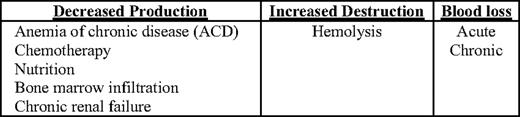
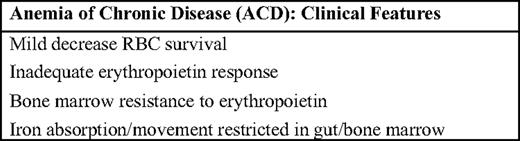
Every anemic patient should have a basic workup to understand the mechanism and cause of the anemia. This workup should include measurements of reticulocytes, creatinine, iron (serum iron, total iron-binding capacity, transferrin saturation, and serum ferritin), B12, and folate. In one study of 261 anemic solid-tumor cancer patients on chemotherapy, 17% had ferritin levels under 100 μg/L, 6% had B12 levels below the laboratory norm, and 2% had creatinine levels above the laboratory norm.1 Another study found that iron studies were not routinely performed in anemic cancer patients and that iron supplementation was rarely given.2 However, the vast majority of anemic cancer patients will have some degree of the anemia of chronic disease (ACD) secondary to their cancer. ACD is mediated by the inflammatory cytokines interferon (IFN)-alpha, -beta, and -gamma; interleukin (IL)-1 and IL-6; and tumor necrosis factor-alpha (TNFα).3 These inflammatory cytokines give ACD its characteristic features (Table 2), which include a mild shortening of red blood cell survival, inadequate erythropoietin response to the degree of anemia and a depressed bone marrow response to the erythropoietin present, and impaired iron availability for the developing red blood cells in the bone marrow (Figure 1).3,4 Hepcidin, a 25-amino-acid molecule manufactured predominantly in the liver, is increased in ACD largely in response to the inflammatory cytokine IL-6. Its principle action is to decrease iron absorption in the duodenum and to trap iron in storage cells, both of which result in decreased iron availability for erythropoiesis.5 Hepcidin levels are conversely decreased by increased erythropoiesis and iron deficiency.6

Multifactorial pathogenesis of anemia in cancer patients. (From Glaspy, 2009.7 Used with permission.) eEPO, endogenous erythropoietin; RE, reticuloendothelial
Multifactorial pathogenesis of anemia in cancer patients. (From Glaspy, 2009.7 Used with permission.) eEPO, endogenous erythropoietin; RE, reticuloendothelial
Laboratory evaluation of ACD would typically reveal a decreased serum iron, decreased total iron binding capacity, decreased transferrin saturation (TSAT), and a normal to increased serum ferritin. Absolute iron deficiency and ACD can occur simultaneously, but diagnosing both in the same patient can be challenging. In the future, hepcidin levels may help make this distinction.
Prevalence of Anemia in the Cancer Patient
How common is anemia in the cancer patient? In the earliest trials of ESAs in anemic cancer patients, 28% of over 300 patients with nonmyeloid malignancy were not only anemic, but required at least one blood transfusion before study entry.8 In a subgroup of patients on cisplatin-based chemotherapy, 44% required blood transfusion, while 26% of patients who did not receive cisplatin chemotherapy required a blood transfusion.9
In a 1999 review of solid-tumor patients on chemotherapy, the incidence of mild to moderate anemia was frequent, with the highest incidence in patients with lymphoma, lung, ovarian, and genitourinary cancers, with a transfusion rate approaching 50% to 60%.10 More recently, in 2004 the European Cancer Anemia Survey study of 15,367 patients at 748 sites in 24 countries found a prevalence of anemia of 39% in cancer patients. During the 6-month survey, 67% became anemic, with the highest incidence (75%) in those receiving chemotherapy. The anemia had a significant effect on World Health Organization (WHO) performance scores, with lower scores being correlated with lower hemoglobin concentrations of 12 g/dL and less.11
Why Treat Anemia in the Cancer Patient?
Anemia can put a strain on an already weakened cancer patient. Cardiac output must increase to maintain adequate oxygen delivery as anemia worsens and symptoms develop. Anemia is also associated with a poorer overall prognosis. Despite all of this, treating the anemic cancer patient is controversial. Blood transfusion can be offered if hemoglobin decreases to a level where symptoms develop or lack of oxygen delivery threatens organs. In these cases, prompt correction of anemia is required. Blood transfusion carries risks, including volume overload, iron overload, and acute and chronic infections. ESAs offer an alternative to transfusion. Higher hemoglobin levels in ESA-treated patients can increase energy, activity, and overall quality of life independently of the cancer response to therapy.12–15 Furthermore, some data suggest that earlier intervention with ESAs before the development of profound anemia can lower the risk of blood transfusion16,17 and further increase quality-of-life scores.18 However, recent studies have raised concern about the safety of ESAs. Following a US Center for Medicare and Medicaid Services National Coverage Decision in 2008 directing that ESAs may not be initiated until hemoglobin levels in chemotherapy-induced anemia (CIA) patients fall below 10 g/dL, blood-transfusion rates have increased in oncology patients.19–21
Given the large number of clinical trials over the last two decades, meta-analyses of ESAs in cancer patients with CIA have examined safety concerns in these patients and under what circumstances they occur. A meta-analysis by Bennett included 51 randomized, controlled trials in 13,611 patients.22 A more recent, independent, patient-level meta-analysis reported by Bohlius included 13,933 cancer patients in 53 randomized, controlled trials.23 These two studies concluded that there was a small but significant decrease in survival in the ESA-treated patients compared with the controls. However, the majority of this safety signal was found in eight trials; in four of these trials, patients were not receiving chemotherapy, and in the other four, the patients were treated with ESA doses and hemoglobin targets that were off-label by North-American and European health agency standards and guidelines. If only those patients treated using government health agency-approved ESA doses and target hemoglobins were included, there was no decrease in overall survival. The latest meta-analysis of 60 trials including 15,323 patients did not show a significant decrease in survival or tumor progression.24 Furthermore, evidence suggests that the greatest risk for a negative impact on survival occurs in those patients whose ESA is continued despite lack of response, especially in patients who not only fail to respond, but also receive a blood transfusion.25,26 All of these trials do show a consistent safety signal regarding venous thromboembolism, with an increased overall risk of about 1.6.27 Of course, a discussion of the safety of ESAs should always be counterbalanced against the safety of a blood transfusion. In addition to the accepted risks of acute reaction or clerical error, there is also the risk of transmitting an unknown infection or even causing immunosuppression, possibly leading to tumor progression, although this latter concern is quite controversial.28
Treatment of CIA
CIA can be managed in several ways. If not severe enough or if the patient is lacking symptoms, it can simply be observed. For symptomatic anemia or if the clinician is concerned by the severity of the anemia, blood transfusion can be given. The US Department of Health and Human Services circular describing circumstances for the proper administration of red-cell transfusions suggests that transfusions should be used for “treatment of symptomatic deficit of oxygen-carrying capacity” and should not be used “to treat anemias that can be corrected with specific medications such as iron, vitamin B12, folic acid, or erythropoietin.”29
The US Food and Drug Administration (FDA) approved recombinant erythropoietin for use in CIA in 1993. The licensing trial by Abels randomized 413 anemic patients with non myeloid malignancy to receive either erythropoietin or placebo for 8 to 12 weeks.30 The patients on chemotherapy received erythropoietin 150 U/kg or placebo subcutaneously 3 times a week for 12 weeks. Hemoglobin response, defined as a correction of hematocrit (HCT) to 38% or more or an increase in HCT of 6 points or more independent of blood transfusion, was significantly greater in the erythropoietin arm than in the placebo arm. Likewise, blood transfusions were less frequent in the erythropoietin arm than in the placebo arm, although this only reached statistical significance in the patients receiving chemotherapy, not in the patients on no chemotherapy, probably because the erythropoietin dose was lower (100 U/kg) and the study duration was shorter (8 weeks instead of 12). Subsequently, darbepoetin was approved by the FDA for CIA in 2001. The licensing trial by Vansteenkiste randomized 320 anemic patients receiving chemotherapy for nonmyeloid malignancies to receive either darbepoetin 2.25 μg/kg or placebo subcutaneously every week. Hemoglobin response, defined here as a hemoglobin increase of 2g/dL or more or achieving 12 g/dL or more, was 66% versus 24%, while blood transfusion was 27% versus 52%, both significantly in favor of darbepoetin.31 Erythropoietin is now also labeled in CIA patients at 40,000 U subcutaneously every week, and darbepoetin is now also labeled at 500 μg subcutaneously every 3 weeks.
In these 60 randomized, controlled trials of either erythropoietin or darbepoetin reported to date, other correctable, treatable causes of anemia, including iron deficiency, are always excluded first, leaving the anemia of ACD and chemotherapy as the only major factors for the ESA to overcome. Even so, all patients do not respond. Hemoglobin responses are usually in the range of 50% to 70%, and no pretreatment predictor or response indicator has yet been identified.32,33
If ACD is due in part to a relative erythropoietin deficiency, then giving higher ESA doses might be expected to improve response rates, but this theory has not met with success.34 Presumably, there comes a point when either higher doses of ESA cannot overcome the bone marrow suppression by inflammatory cytokines, or whatever iron is available in storage in the bone marrow or elsewhere can no longer meet the erythropoietin-driven demand for erythropoiesis.
Iron Availability
This leads to the discussion of iron availability in the CIA patient receiving ESA. If ACD is a combination of inadequate erythropoietin response to the degree of anemia and iron-restricted erythropoiesis due to inflammatory cytokines and hepcidin, then why not give both exogenous erythropoietin and iron? Furthermore, because oral iron is poorly absorbed in ACD, as discussed above, why not give IV iron? In theory, then, those patients who have the most significant iron-restricted erythropoiesis would be the ones most likely to respond to IV iron. Two laboratory parameters, reticulocyte hemoglobin content and percent hypochromic red blood cells, indicate when and how significant iron-restricted erythropoiesis occurs, but these two tests are not readily available in clinical laboratories.35 Currently, a serum ferritin greater than 20 μg/L, a TSAT less than 20%, and serum iron less than 60 μg/dL provide a useful definition of functional iron deficiency or, more correctly, iron-restricted erythropoiesis.36
This all leaves one nagging question. If the body stores of iron are subjected to the reticuloendothelial system “lock” of inflammatory cytokines in ACD, wouldn't the same thing be true of the additional iron given IV? So, as discussed below, why does IV iron generally enhance the response to ESA in anemic cancer patients on chemotherapy? This question remains unanswered, but a working hypothesis is that the reticuloendothelial system “lock” is not 100% and probably can be overwhelmed by giving more iron, allowing some leakage to occur and augmenting erythropoiesis. In addition, a very small amount of the IV iron infused may go directly to bind transferrin, bypassing macrophages, and may also help to relieve iron-restricted erythropoiesis.37
Studies of Intravenous Iron in Nephrology
ESA use in chronic kidney disease patients on hemodialysis has caused dramatic reductions in the need for blood transfusion and an associated improvement in maintenance hemoglobins without the need for transfusion. Iron supplementation is obviously necessary in iron-deficient patients, but IV iron also improves ESA response in the iron-replete patient by relieving iron-restricted erythropoiesis.
The DRIVE (Dialysis patients' Response to IV iron with Elevated ferritin) study examined 134 anemic chronic kidney disease patients on hemodialysis receiving ESA with ferritin levels of 500 to 1200 μg/L and TSAT of 25% or under. Patients either received 1g of IV ferric gluconate in eight divided doses or no iron. Hemoglobins increased more and faster in the IV iron group, independent of baseline ferritin or TSAT,38 with significant reductions in ESA usage.39
Studies of IV Iron in Oncology
Nine prospective randomized, controlled trials have compared IV iron to oral iron or no iron in CIA patients receiving ESAs.40–48 Hemoglobin change was the primary outcome parameter in eight studies, while transfusion outcome was the primary end point in the other one.43 Eight of the nine studies demonstrated an increase in hemoglobin/hematopoietic response, shorter time to response, decreased ESA exposure, or decrease in blood transfusion when IV iron was added. Only one of the nine studies failed to show an advantage to giving IV iron.48 Mean pretreatment ferritin levels in these nine trials ranged from 160 to 460 μg/L (range 10–1000), and mean pretreatment TSATs ranged from 19% to 36% (range 15%–0%) (Table 3).
Studies evaluating IV iron and ESA in oncology
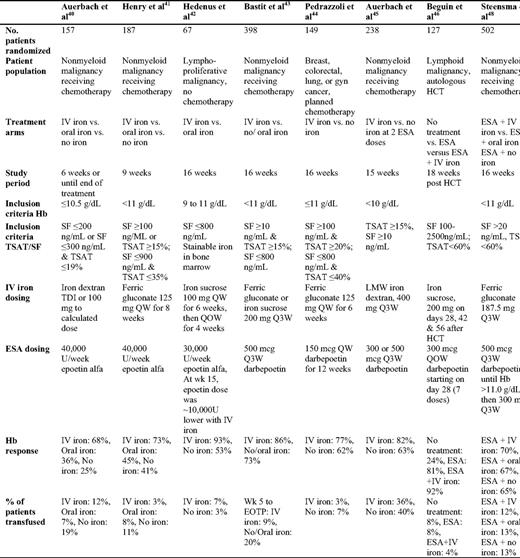
(Modified from Auerbach and Glaspy, 200949 Used with permission.)
HCT, hematopoietic stem cell transplantation; TSAT, transferrin saturation; SF, serum ferritin; TDI, total dose infusion; QW, once a week; Q3W, once every 3 weeks; QOW, once every other week
The studies vary in some of their baseline iron characteristics and outcome measurements. Bastit demonstrated a significant decrease in the number of blood transfusions in the patients receiving both ESA and IV iron compared with ESA alone.43 Pedrazzoli excluded patients with both absolute and/or functional iron deficiency by requiring an initial ferritin greater than 100 μg/L and a TSAT greater than or equal to 20%. Even in these arguably iron-replete patients, hemoglobin responses were significantly better in the ESA- and IV iron-treated patients.44 Auerbach demonstrated ESA dose sparing in his study, in which patients received either no iron or IV iron with darbepoetin 300 or 500 μg subcutaneously every 3 weeks.45 Hemoglobin responses were significantly better in the IV iron arm at the lower dose of darbepoetin of 300 μg than at the higher dose of 500 μg without the IV iron. ESAs for anemic patients after autologous bone marrow transplant have not proven very helpful in studies in which the ESA is begun less than 30 d after bone marrow transplantation.50 However, in a study by Beguin, there was a significant increase in the hemoglobin in bone marrow transplant patients given both IV iron and ESA versus ESA alone when this treatment was initiated in patients whose anemia was still present 30 d or more after bone marrow transplant.46 Interestingly, in all seven of these trials with hemoglobin as their primary outcome variable, the benefit was independent of the baseline iron parameters, although there was a trend toward better response rates in those patients with initial TSATs under 20%.40,41
The most recent IV iron study by Steensma randomized CIA patients on darbepoetin to receive no iron, oral iron, or IV iron with ferric gluconate 187.5 mg IV every 3 weeks for 15 weeks.48 Average baseline ferritin levels were 456 to 479 μg/L, and average baseline TSATs were 19.6% to 22.5%. The primary study end point was hemoglobin change, and there were no significant differences among the three treatment arms. Of the nine IV iron trials in CIA patients on ESA, this was the only study that did not demonstrate the superiority of IV iron. How can this be explained? With the exception of the hematopoietic stem-cell transplant study by Beguin, which looked at a different patient population, the study by Steensma delivered the lowest dose rate of IV iron of any of the studies. For example, after 3 weeks only 187.5 mg of IV iron was administered, while in all of the other studies, patients had received almost twice as much iron by 3 weeks. A study in chronic kidney disease hemodialysis patients on ESA suggests that a minimum amount of IV iron must be given in order to make a difference. In this trial, a dose of IV ferric gluconate of 500 mg versus 1000 mg was given in eight divided doses over consecutive dialysis sessions and compared against a group receiving oral iron as the control.51 The 1000 mg IV iron group had significantly higher hemoglobin levels, ferritin levels, and TSATs at all follow-up time points. The 500 mg IV iron group was no different than the oral iron controls. When giving IV iron, mean ferritin would be expected to rise the most in the IV iron arm and rise the least or fall in the other arms, and TSATs would be expected to fall most dramatically in the oral/no iron arms and less so in the IV iron arms as the ESA drives erythropoiesis.41 Perhaps indicative of this lower IV iron dosing rate in the Steensma study, the TSATs increased in all three arms, but increased the highest in the oral iron arm, contrary to what would be expected. The ferritin levels did increase in the IV iron arm and remained almost flat in the oral and placebo arms. These data would suggest that there was no iron-restricted erythropoiesis in any of the study arms, which, again, is contrary to what would be expected. Nevertheless, this was a well-conducted, randomized, controlled trial and its negative results need to be factored in when considering all nine trials.
What about giving IV iron to CIA patients on ESA, but only if they do not respond to standard dosing ESA therapy first or, even more interesting, what about just giving CIA patients IV iron without ESAs at all? In a study by Bellet, 375 CIA patients were randomized to receive ESA alone during the first 8 weeks.47 Patients were classified as non-responders or responders based on a hemoglobin increase of 1 g/dL or not. Then, for the next 12 weeks, both responders and non-responders received either 1500 mg of IV iron sucrose in three divided doses or not. Interestingly, both non-responders and responders who got the IV iron had significantly greater hemoglobin responses than those who did not receive the IV iron.
In a study by Kim, 75 patients with cervical cancer were randomized to receive either 200 mg of IV iron sucrose weekly (n = 30) or not (n = 45) along with their radiation and weekly cisplatin chemotherapy.52 No ESA was given. No baseline or on study iron parameters were provided; nevertheless, there was a significant difference in blood transfusions between the IV iron patients (40%) and the control patients (64%). In another study by Dangsuvan, 44 anemic gynecologic cancer patients receiving chemotherapy were randomized after a first transfusion to subsequently receive either iron sucrose 200 mg IV or oral iron, again without ESA. Subsequent transfusions were 22.7% in the IV iron group and 63.6% in the oral iron group.53 No baseline or on study iron parameters were available in this study either. To date, these are the only studies that have attempted to ask the question whether CIA patients can correct their anemia with IV iron alone without ESA. Clearly, this question needs to be answered, and other studies employing only IV iron are planned.
The National Comprehensive Cancer Network guidelines currently recommend a laboratory screening evaluation for all patients symptomatic of anemia or who risk developing symptomatic anemia from CIA when hemoglobin falls below 11 g/dL. IV iron can be considered in such patients if absolute iron deficiency (ferritin < 30 μg/L, TSAT < 15%) or iron-restricted erythropoiesis (ferritin ≤ 800 μg/L, TSAT < 20%) is present. The American Society of Clinical Oncology also recommends initial and periodic monitoring of iron parameters in CIA patients on ESA, and suggests that iron repletion may help limit the need for ESA while maximizing symptomatic improvement, although the dose, route, and frequency of iron administration were not specified.54
Summary
Anemia is common in cancer patients. Its cause is multifactorial and a brief workup should always be undertaken to rule out simple, reversible causes. ACD and CIA are the most likely causes of anemia. Symptomatic or clinically severe anemia may require treatment with blood transfusion or ESA. If ESA therapy is chosen, developing evidence suggests that the addition of IV iron can limit iron-restricted erythropoiesis, even in the iron-replete patient, and improve the response to ESA.
Disclosure
Conflict-of-interest disclosure: Speakers' bureau, research funding, and membership on the board of directors or advisory committees of Amgen, OrthoBiotech, and Watson Pharma.
Off-label drug use: Ferrlecit, Venofer, and Infed are not labeled for use in anemic cancer patients on chemotherapy receiving ESAs.
Correspondence
David H. Henry, MD, Joan Karnell Cancer Center at Pennsylvania Hospital, 230 West Washington Square, 2nd floor, Philadelphia, PA 19106; Phone: 215-829-6311; Fax: 215-829-6104; e-mail: davidhenry@pennoncology.com
