
Introduction
A 52-year-old avid tennis player develops an idiopathic left lower extremity deep vein thrombosis. She has no medical problems except for hypertension. She is up to date with her age-specific cancer screening. She had a negative colonoscopy at age 50 and a recent mammogram and Pap smear with no concerning findings. She read that clots may be the first manifestation of cancer and she wonders if she needs an extensive workup to look for a hidden cancer.
The association between cancer and thrombosis was first proposed by Armand Trousseau when he recognized the condition of thrombophlebitis migrans as a forewarning of occult malignancy.1 Venous thromboembolism (VTE) is a common complication in patients with cancer,2–4 and it may be the first clinical presentation of an occult malignancy. Approximately 10% of patients who present with an idiopathic or unprovoked VTE are diagnosed with cancer within the next 1 to 2 years.5–9 These provocative findings raise the question as to whether all patients with idiopathic VTE should undergo extensive screening to look for occult cancer.10
To examine the current best evidence for this question, we performed a comprehensive computerized literature search of the OVID database using the terms thrombosis (Medical Subject Headings [MeSH] search including venous thrombosis, pulmonary embolism [PE], deep vein thrombosis [DVT], venous thromboembolic events, thromboembolism, and venous thromboembolism, with 156267 hits) AND neoplasms (MeSH including cancer, malignancy, tumor, and occult malignancy, with 1604571 hits) AND screening (MeSH including screen, search, early detection, and early diagnosis, with 469301 hits) between 1950 and week 1 of July 2010. This strategy provided 584 total hits. Additional studies were gleaned from the reference lists of the relevant studies. After reviewing the database for case reports, case series, and prospective, retrospective, and randomized, controlled trials, more than 40 studies were identified that addressed screening for occult malignancy in patients with VTE.
For this mini-review, we focus on key randomized, controlled and prospective studies. The characteristics of these studies are summarized in Table 1. Most studies reported excluding patients with known or prior cancers.11–14,16,17,19 Only two studies directly compared limited versus extensive screening strategies.17,18
Summary of randomized trials and prospective studies reporting the incidence of unknown cancer detected with screening and during follow up in patients presenting with VTE
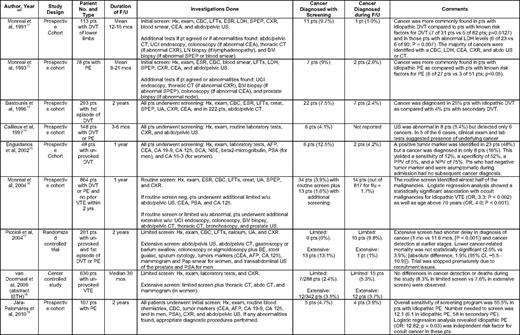
Abdo, abdomen; AFP, alphafetoprotein; BE, barium enema; BM, bone marrow; CA, carbohydrate antigen; CEA, carcinoembryonic antigen; CBC, complete blood count; CI, confidence interval; creat, creatinine; CRP, C-reactive protein; CXR, chest radiography; DVT, deep vein thrombosis; ESR, erythrocyte sedimentation rate; f/u, follow up; Hx, history; LDH, lactic dehydrogenase; LFTs, liver function tests; LN, lymph node; mos, months; neg, negative; No., number; NSE, neuron-specific enolase; OR, odds ratio; PE, pulmonary embolus; NPV, negative predictive value; PPV, positive predictive value; PSA, prostate specific antigen; pts, patients; SCC, squamous-cell antigen; SPEP, serum protein electrophoresis; UA, urinanalysis; UGI, upper gastrointestinal; US, ultrasound; vs, versus; VTE, venous thromboembolism; w/u, work up; yrs, years
Based on this review, we conclude that patients with idiopathic VTE are at an increased risk of harboring an occult cancer compared with patients with provoked VTE. Furthermore, a thorough history, physical examination, routine blood tests, and chest X-ray detected many of the cancers. An extensive search appeared to detect more cancers and at earlier stages than a limited search. However, even with extensive screening, up to one-third of cancers were missed. Careful patient selection, such as older patients with anemia or bilateral VTE, may increase this yield.
It remains unclear whether earlier cancer detection in patients with idiopathic VTE changes the prognosis or improves overall outcome, including morbidity, mortality, and quality of life. The only randomized, controlled trial designed to address this question failed to show a positive impact on cancer-related survival, but the study was underpowered, had methodological limitations, and may have been guilty of lead-time bias.17 Another argument against extensive screening is that it carries both economical and psychological costs and may cause harm. It is important to keep in mind that without effective anticancer therapies, screening and detection in and of itself cannot improve overall survival. Thus, well-designed, large, randomized clinical trials are needed to evaluate the benefit and costs of extensive screening for occult cancers in patients with idiopathic VTE.
Based on the available studies, we recommend that clinicians maintain a low threshold of suspicion for malignancy in patients who present with an unprovoked VTE. Moreover, patients with unprovoked VTE should provide a thorough medical history, undergo a physical examination, chest X-ray, and routine laboratory tests (including complete blood count, basic chemistries, liver function, and lactate dehydrogenase), and be up to date with age- and gender-specific cancer screening (Grade 1C). Additional diagnostic testing should be guided by any abnormal findings gleaned from the initial clinical or laboratory data.
Disclosure
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Off-label drug use: None disclosed.
Correspondence
Dr. Agnes Y.Y. Lee, Diamond Health Care Centre, 2775 Laurel Street, 10th floor, Vancouver, BC, Canada V5Z 1M9; Phone: (604) 875-4592; Fax: (604) 875-4696; e-mail: alee14@bccancer.bc.ca
