
Page 578: The title of the article should be “Noninfectious lung complications of hematopoietic cell transplantation.” The word “lung” was omitted from the title in the original publication.
Page 583: In the left part of Figure 2, “hypotension” should read “hypertension.” The corrected figure is shown below.
The errors have been corrected in the published article.
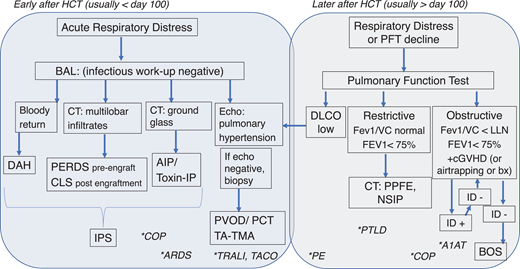
Flow diagram for workup and diagnosis of noninfectious lung diseases after HCT.Blue box, diseases commonly diagnosed in the first 100 days after HCT. Gray box, those diseases occurring usually beyond day 100 after HCT. Noninfectious lung injury workup and diagnoses are in boxes. *Additional pulmonary diagnoses are denoted by stars and listed in the column in which these diagnoses would be included in the differential. Notably, other processes can exhibit low DLCO, which is often reduced in RLD, but isolated DLCO reduction should prompt evaluation for vascular diseases of the lung. For the workup of obstructive disease, infection is often diagnosed, which should prompt repeat testing after treatment to ascertain BOS diagnosis (arrows). bx, biopsy; DLCO, diffusion capacity of lung for carbon monoxide; ID, infectious disease workup; PE, pulmonary embolism; toxin-IP, toxin associated interstitial pneumonitis, including that from radiation or chemotherapy.
Flow diagram for workup and diagnosis of noninfectious lung diseases after HCT.Blue box, diseases commonly diagnosed in the first 100 days after HCT. Gray box, those diseases occurring usually beyond day 100 after HCT. Noninfectious lung injury workup and diagnoses are in boxes. *Additional pulmonary diagnoses are denoted by stars and listed in the column in which these diagnoses would be included in the differential. Notably, other processes can exhibit low DLCO, which is often reduced in RLD, but isolated DLCO reduction should prompt evaluation for vascular diseases of the lung. For the workup of obstructive disease, infection is often diagnosed, which should prompt repeat testing after treatment to ascertain BOS diagnosis (arrows). bx, biopsy; DLCO, diffusion capacity of lung for carbon monoxide; ID, infectious disease workup; PE, pulmonary embolism; toxin-IP, toxin associated interstitial pneumonitis, including that from radiation or chemotherapy.
