

Abstract
Unlike younger adults with acute lymphoblastic leukemia (ALL), older adults are rarely cured due to a combination of intrinsic disease resistance and treatment-related toxicities. Novel therapeutics such as inotuzumab ozogamicin, blinatumomab, venetoclax, and ABL kinase inhibitors have high activity in ALL and are well tolerated by older adults. Frontline treatment regimens for older adults using novel therapeutics with reduction or omission of conventional chemotherapy are being developed with early results demonstrating high remission rates and lower toxicity, but long-term efficacy and toxicity data are lacking. Collaboration between academic and pharmaceutical stakeholders is needed to develop clinical trials to define the optimal treatment regimens for older adults with ALL.
Learning Objectives
Understand the role of novel therapeutics vs CC in initial treatment of older adults with Ph-negative ALL
Understand the role of tyrosine kinase inhibitor treatment with or without CC or novel therapeutics in initial treatment of adults with Ph-positive ALL
Outcomes of older adults in the era of conventional chemotherapy
For most of history, acute lymphoblastic leukemia (ALL) has been an uncompromising, deadly illness regardless of age, comorbidities, or social circumstance. Then, in 1948, Sidney Farber announced 5 temporary remissions among 16 children with acute leukemia treated with the folic acid antagonist, aminopterin.1 Now, after decades of effort by numerous clinicians, scientists, and cooperative groups, more than 90% of children in resourced settings are cured of ALL with chemotherapy.2 Although celebrated, these pediatric ALL chemotherapy regimens are notable for length, complexity, and toxicity.
Traditionally thought of as a pediatric disease, approximately half of ALL diagnoses occur in younger (18-49 years) and older (≥50 years) adults in roughly equal porportions.3 Unfortunately, the outstanding outcomes in children have not been replicated in older cohorts. The standard approach to treating ALL in adults has been conventional chemotherapy (CC) programs adapted from pediatric schedules but with more myelosuppressive agents and a deemphasis on the noncytotoxic agents that feature prominently in pediatric regimens (corticosteroids, vincristine, and asparaginase). Results in young adults have improved due to the use of pediatric-like therapy, with more than 70% now achieving long-term survival, but older adults aged 55 to 60 or more years have consistently fared more poorly, with less than 20% cured (Table 1).4-9 Older patients experience more toxicity, leading to dose reductions, treatment delays, and high rates of early death and treatment-related mortality in remission.4-7,11,12 In addition, high-risk genetic features are more common, leading to fewer remissions and frequent relapse.10,16 Age-based dose modifications and prospective studies of CC designed specifically for older adults have not improved outcomes.4,5,12-14,17 There remains no accepted standard-of-care CC regimen for older adults with ALL.
Outcomes of older adults treated with CC, select trials (see also Gökbuget10 )
| Trial | Age, y | N | CR, % | Early mortality,% | OS, % (95% CI) | Death in CR, among those achieving CR, % |
|---|---|---|---|---|---|---|
| Adult trials, outcomes by age | ||||||
| CALGB 91115 | All | 185 | 85 | 8 | 3 years: 43 (36-50) | 8 |
| ≥60 | 35 | 77 | 17 | 17 (9-31) | — | |
| 30-59 | 42 | 84 | — | 40 (30-51) | — | |
| <30 | 39 | 90 | — | 57 (46-68) | — | |
| ECOG 2993/UKALL XII7,11 | 55-65 | 100 | 73 | 18 | 5 years: 21 (12-20) | 23 |
| <55 | 1814 | 93 | 4 | 41 (39-43) | — | |
| Hyper-CVAD12 | ≥60 | 122 | 84 | 10 | 5 years: 20 | 34 |
| <60 | 409 | 92 | 2 | 48 | 7 | |
| Prospectively designed for older adults | ||||||
| DFCI regimen13 | 51-75 | 30 | 67 | 13 | 2 years: 52 (33-68) | — |
| 60-75 | 13 | 76 | — | 70 (42-86) | ||
| 51-59 | 17 | 58 | — | 31 (10-55) | ||
| GMALL14 | 55-85 | 268 | 76 | 14 | 5 years: 23 | 6 |
| 55-65 | — | — | 7 | — | — | |
| 65-75 | — | — | 14 | — | — | |
| ≥75 | — | — | 37 | — | — | |
| PETHEMA ALLOLD0715 | >55 | 56 | 74 | 13 | 32 (at last follow-up, median 11.4 months) | 3 |
| Trial | Age, y | N | CR, % | Early mortality,% | OS, % (95% CI) | Death in CR, among those achieving CR, % |
|---|---|---|---|---|---|---|
| Adult trials, outcomes by age | ||||||
| CALGB 91115 | All | 185 | 85 | 8 | 3 years: 43 (36-50) | 8 |
| ≥60 | 35 | 77 | 17 | 17 (9-31) | — | |
| 30-59 | 42 | 84 | — | 40 (30-51) | — | |
| <30 | 39 | 90 | — | 57 (46-68) | — | |
| ECOG 2993/UKALL XII7,11 | 55-65 | 100 | 73 | 18 | 5 years: 21 (12-20) | 23 |
| <55 | 1814 | 93 | 4 | 41 (39-43) | — | |
| Hyper-CVAD12 | ≥60 | 122 | 84 | 10 | 5 years: 20 | 34 |
| <60 | 409 | 92 | 2 | 48 | 7 | |
| Prospectively designed for older adults | ||||||
| DFCI regimen13 | 51-75 | 30 | 67 | 13 | 2 years: 52 (33-68) | — |
| 60-75 | 13 | 76 | — | 70 (42-86) | ||
| 51-59 | 17 | 58 | — | 31 (10-55) | ||
| GMALL14 | 55-85 | 268 | 76 | 14 | 5 years: 23 | 6 |
| 55-65 | — | — | 7 | — | — | |
| 65-75 | — | — | 14 | — | — | |
| ≥75 | — | — | 37 | — | — | |
| PETHEMA ALLOLD0715 | >55 | 56 | 74 | 13 | 32 (at last follow-up, median 11.4 months) | 3 |
DFCI, Dana-Farber Cancer Institute.
Clinicians caring for older adults with ALL perceive limited benefit of CC. A 2019 US Medicare analysis revealed that only 53.5% of patients with ALL aged 66 or more years received any treatment within 90 days of diagnosis.18 A 2017 US Surveillance, Epidemiology, and End Results analysis reported a median overall survival (OS) of just 4 months among adults 60 years or older diagnosed with ALL since 1980, with minimal progress over 3 decades (3-year OS increasing from 10% to 16%).19 In summary, the chemotherapy regimens that cure children are not a good match for older adults.10,16
Novel approaches to Philadelphia chromosome–negative ALL in older adults
CASE 1
A 78-year-old man with coronary artery disease, hypertension, and hyperlipidemia developed several weeks of fatigue and weight loss. Prior to illness, he visited the gym regularly engaging in vigorous exercise. Laboratory work revealed pancytopenia (white blood cell count, 2.9 K/µL; hemoglobin, 11.2 g/dL; platelets, 86 K/µL) with 7% circulating blasts. He was diagnosed with B-cell acute lymphoblastic leukemia (B-ALL). Immunophenotype was CD45+, CD34+, HLA-DR+, TdT+, CD19+ (variable), CD22+, CD10−, and CD20−. Karyotype was complex with no evidence of the Philadelphia chromosome. Next-generation sequencing revealed a pathogenic mutation in TP53. In 2019, he was referred to our academic center.
The development of novel chemotherapy agents—blinatumomab and inotuzumab ozogamicin (IO)—for relapsed B-ALL has led to a reimagining of the treatment for older adults with ALL. IO is a CD22 monoclonal antibody covalently linked to calicheamicin, a cytotoxic agent (antibody–drug conjugate). Blinatumomab is a bispecific T-cell engager targeting CD19 and CD3. Each is now approved by the US Food and Drug Administration (FDA) for relapsed and refractory (R/R) ALL based on phase 3 randomized trial data showing superiority of the novel agent to salvage cytotoxic chemotherapy in the R/R setting.20,21 It is hoped that using IO and blinatumomab in the first-line treatment of older adults will allow toxic CC to be de-escalated or omitted, resulting in both improved response rates and less toxicity.
IO plus CC
Investigators at MD Anderson Cancer Center (MDACC) have been testing IO plus mini-hyper-CVD (cyclophosphamide, vincristine, dexamethasone), a lower-intensity CC regimen, in older adults (≥60 years) with untreated Philadelphia chromosome–negative (Ph–) CD22+ B-ALL in a single-center phase 2 trial (NCT01371630, Table 2). In the original design, IO was administered on day 3 of the first 4 of 8 planned CC cycles followed by 36 months of POMP (6-mercaptopurine, vincristine, methotrexate, prednisone) maintenance. In 2018, MDACC investigators reported high response rates (98% overall response rate [ORR], 96% minimal residual disease-negativity [MRD-negativity]) and no early mortality in the first 52 patients treated.22 An update of the trial in 2020 (with 70 patients enrolled) was notable for continued high response rates (98% ORR, 96% MRD negativity, with no early deaths) and an encouraging 3-year complete remission (CR) duration and OS of 79% and 56%, respectively.23
Novel approaches to Ph– ALL in older adults: published and ongoing trials*
| Reference | Regimen | Phase | N | Line | Age, y | Regimen-related deaths | Response | Survival |
|---|---|---|---|---|---|---|---|---|
| Kantarjian et al (2018)22 Short et al (2020)23 NCT01371630 | IO + mini-hyper-CVD (Blina consolidation) | 2 | 70 | First | ≥60 | 0% early mortality 34% mortality in remission | 98% ORR 88% CR (96% MRD negative) | Continuous CR 3 years: 79% Median CCR NR OS 3 years: 56% Median OS 62 months |
| EWALL-INO NCT03249870 | IO + mild-intensity chemotherapy CC consolidation | 2 | — | First | ≥55 | — | — | — |
| Stelljes et al (2020)24 GMALL (INITIAL-1) NCT03460522 | IO induction CC consolidation | 2 | 36 | First | ≥56 | 0% early mortality | 100% CR/CRi (78% MRD negative) | EFS 1 year: 87% (95% CI, 70-100) OS 1 year: 87% (95% CI, 70-100) |
| Jain et al (2019)25 DFCI/MDACC IST NCT03319901 | Venetoclax + mini-hyper-CVD | 1b/2 | 19 | R/R (8) First (11) | All ages ≥60 | 0% early mortality | 91% CR (100% MRD negative) | — |
| Advani et al (2018)26 SWOG 1318 NCT02143414 | Blina induction Blina consolidation | 2 | 29 | First | ≥65 | 0% | 66% CR/CRi (92% MRD negative) | DFS 1 year: 56% (95% CI, 58-90) OS 1 year: 65% (95% CI, 43-80) |
| Alliance 041703 NCT03739814 | IO induction Blina consolidation | 2 | — | R/R First | All ages ≥60 | Results pending | Results pending | Results pending |
| Reference | Regimen | Phase | N | Line | Age, y | Regimen-related deaths | Response | Survival |
|---|---|---|---|---|---|---|---|---|
| Kantarjian et al (2018)22 Short et al (2020)23 NCT01371630 | IO + mini-hyper-CVD (Blina consolidation) | 2 | 70 | First | ≥60 | 0% early mortality 34% mortality in remission | 98% ORR 88% CR (96% MRD negative) | Continuous CR 3 years: 79% Median CCR NR OS 3 years: 56% Median OS 62 months |
| EWALL-INO NCT03249870 | IO + mild-intensity chemotherapy CC consolidation | 2 | — | First | ≥55 | — | — | — |
| Stelljes et al (2020)24 GMALL (INITIAL-1) NCT03460522 | IO induction CC consolidation | 2 | 36 | First | ≥56 | 0% early mortality | 100% CR/CRi (78% MRD negative) | EFS 1 year: 87% (95% CI, 70-100) OS 1 year: 87% (95% CI, 70-100) |
| Jain et al (2019)25 DFCI/MDACC IST NCT03319901 | Venetoclax + mini-hyper-CVD | 1b/2 | 19 | R/R (8) First (11) | All ages ≥60 | 0% early mortality | 91% CR (100% MRD negative) | — |
| Advani et al (2018)26 SWOG 1318 NCT02143414 | Blina induction Blina consolidation | 2 | 29 | First | ≥65 | 0% | 66% CR/CRi (92% MRD negative) | DFS 1 year: 56% (95% CI, 58-90) OS 1 year: 65% (95% CI, 43-80) |
| Alliance 041703 NCT03739814 | IO induction Blina consolidation | 2 | — | R/R First | All ages ≥60 | Results pending | Results pending | Results pending |
Results at most recent publication.
Blina, blinatumomab; CCR, continuous complete remission; CRi, complete remission with incomplete count recovery; NR, not reached.
Notable toxicities associated with the IO plus mini-hyper-CVD regimen have included frequent prolonged thrombocytopenia (81%), hepatotoxicity (17% grade ≥3 hyperbilirubinemia, 9% veno-occlusive disease), and infections (41% during induction, 70% during consolidation).23 Death in remission due to treatment-related toxicity has been the major challenge. At the most recent update, 34% (24/70) of responding patients had died in CR due to sepsis, veno-occlusive disease, or secondary myeloid malignancies. Mortality was more common in patients 70 years or older who comprised ~40% of enrolled patients. In response to an initial experience with toxicity, protocol modifications have included IO dose fractionation and reduction (to address liver toxicity) and a drastic decrease in the number of recommended CC cycles (originally 8, decreased to 4 for patients aged 60-69 years and to 2 for patients aged ≥70 years).
The European phase 2 EWALL (European Working Group for Adult ALL)-INO study (NCT03249870) is also exploring IO in combination with low-intensity chemotherapy for untreated patients 55 years or older with CD22+ ALL. Patients receive IO plus low-intensity chemotherapy induction for 2 cycles followed by IO-free chemotherapy consolidation and maintenance.
In contrast to the combination approach taken by MDACC and EWALL, the German Multicenter Study Group for Adult Acute Lymphoblastic Leukemia (GMALL) study group is studying a sequential approach. In the phase 2 INITIAL-1 study (NCT03460522), untreated older adults (aged >55 years) receive 3 cycles of IO monotherapy followed by CC consolidation (Table 2). A 100% CR was reported among the first 31 patients treated (78% MRD negative), with the majority (29/31) able to complete all 3 IO induction cycles with no early deaths.24 Long-term efficacy and toxicity of the regimen are not yet known.
Venetoclax plus CC
The BCL2 inhibitor venetoclax, an agent with demonstrated preclinical and clinical activity in relapsed ALL, is also being studied in the frontline in combination with mini-hyper-CVD (NCT03319901, Table 2).27,28 A phase 1b study of venetoclax plus mini-hyper-CVD for relapsed/refractory (R/R) (n = 8) and newly diagnosed patients 60 years or older (n = 11) with ALL demonstrated safety (no dose-limiting toxicities (DLTs) or early mortality), with venetoclax 600 mg daily declared the recommended phase 2 dose.25 Notably, there was no evidence of prolonged cytopenias or liver toxicity. The regimen was particularly effective in newly diagnosed patients, with 91% (10/11) achieving an MRD-negative CR, including 6 patients with a TP53 mutation. Because 9 of 10 responders were consolidated with allogeneic hematopoietic stem cell transplant (HSCT), there are limited data on late toxicity. The trial has now moved to phase 2 (with venetoclax 400 mg) and is currently enrolling adults 60 years or older with newly diagnosed Ph– ALL. A distinct advantage of this regimen is that it can be offered to patients with both B- and T-cell ALL, in contrast to approaches that rely on B-lineage restricted antibodies and antibody–drug conjugates. Venetoclax is not approved by the FDA for ALL.
Closing the curtain on chemotherapy for Ph– ALL?
Given the efficacy of novel agents, a chemotherapy-free approach may be possible. The US National Clinical Trial Network (NCTN) trial Southwest Oncology Group (SWOG) 1318 phase 2 study of blinatumomab induction followed by blinatumomab consolidation for newly diagnosed Ph– B-ALL (aged >65 years) reported a 66% CR rate (92% MRD negative) among the first 29 patients with no early deaths (NCT02143414, Table 2).26 Another phase 2 NCTN trial (Alliance 041703 NCT03739814) is investigating IO induction followed by blinatumomab consolidation (Table 2). This approach seeks to use each novel agent to maximum advantage. IO is active regardless of disease burden, making it an ideal induction agent, whereas blinatumomab is more effective and less toxic in settings of lower disease burden and thus a good agent for consolidation therapy.15,29
Encore for chemotherapy
Blinatumomab and IO achieve high response rates in the R/R setting but with short durability.20,21 Although the durability of single-agent novel therapy in the upfront setting is not known, relapses driven by selective pressure would be expected. It is hypothesized that low-intensity CC integrated into induction and/or consolidation (as being pursued by EWALL-INO and GMALL INITIAL-1 studies) may continue to benefit older patients receiving novel agents by applying broader antileukemic pressure and diminishing opportunities for clonal escape. Novel combination approaches (such as being studied in A041703) may offer the best of both worlds via a multipronged attack without chemotherapy toxicities. MDACC has added blinatumomab consolidation to their IO plus mini-hyper-CVD protocol. Venetoclax plus IO will also soon be tested in R/R B-ALL due to nonoverlapping toxicities and preclinical evidence for synergy.30 If shown to be safe, it may be useful as a frontline regimen. For T-cell ALL, a chemotherapy-free option does not yet exist. More research to identify therapeutic vulnerabilities and novel therapeutics for this subtype is needed.
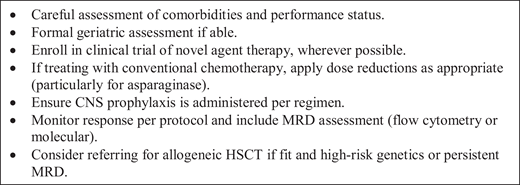
CASE 1 (continued)
The patient was treated with venetoclax plus mini-hyper-CVD on an investigational protocol and achieved an MRD-negative CR after 1 cycle. He completed 4 cycles of venetoclax plus mini-hyper-CVD, after which he was bridged to venetoclax plus POMP maintenance due to toxicity from CC. He continued POMP maintenance for 2 years and remains in an ongoing remission. (See Figure 1 for approach to Ph– ALL in older adults.)
Novel approaches to Ph+ ALL in older adults
CASE 2
A 73-year-old woman with a history of hypertension and rheumatoid arthritis was asymptomatic but found to have an abnormal complete blood count on routine testing: white blood cells (19 K/µL) with 39% circulating blasts that are CD45+, CD34+, HLA-DR+, TdT+, CD19+, CD10+, and CD20−. Karyotype shows t(9;22) with additional abnormalities. Reverse transcription polymerase chain reaction shows p210 transcript more than 50% international scale (IS).
The Philadelphia chromosome is present in approximately half of ALLs in older adults.31 Historically associated with an adverse prognosis, the development of ABL kinase inhibitors has resulted in frequent cures in younger adults and in older adults has enabled prolonged remissions, negating the adverse prognosis.32-34 Older adults with ALL are ideal candidates for low-intensity CC and chemotherapy-free tyrosine kinase inhibitor (TKI)–based protocols.
TKI plus CC
The EWALL has studied TKI plus low-intensity CC in adults 55 years or older (NCT028889777, Table 3). Second-generation TKIs were combined with low-intensity induction and consolidation CC in the consecutive EWALL-PH01 (dasatinib) and EWALL-PH02 (nilotinib) protocols. Both protocols resulted in high CR rates (>95%) without induction mortality. Long-term survival was particularly encouraging in the EWALL-PH02, in which allogeneic HSCT was pursued in 30% (24/79) of patients (4-year OS, 47%; 61% and 39% in transplanted vs nontransplanted, respectively).35,36 Importantly, the Group for Research on Adult Acute Lymphoblastic Leukemia (GRAAPH)-2005 trial, which enrolled younger adults (18-59 years), demonstrated that reduced-intensity CC induction was associated with fewer induction deaths and equivalent efficacy compared with standard-intensity CC induction, questioning the benefit of intensive CC induction for any patient (regardless of age) with Ph+ ALL in the TKI era.37
Novel approaches to Ph+ ALL in older adults: published and ongoing trials*
| Reference | Regimen | Phase | N | Line | Age, y | Regimen- related deaths | Response | Survival |
|---|---|---|---|---|---|---|---|---|
| Rousselot et al (2016)35 EWALL PH-01 NCT028889777 | Dasatinib 140 mg daily + low-intensity CC | 2 | 71 | First | ≥55 | 4% (3/71) induction 12% (6/71) treatment-related mortality in CR | 96% CR 65% 3-log reduction in BCR-ABL | 27% (95% CI, 17-37) 5-year EFS 36% (95% CI, 25-47) 5-year OS 7 received HSCT 75% of relapses T315I |
| Ottmann et al (2018)36 EWALL PH-02 NCT028889777 | Nilotinib 400 mg twice daily + low-intensity CC | 2 | 79 | First | ≥55 | 1% (1/79) induction 11 died in CR (6 after HSCT) | 94.4% CR | 42% 4-year EFS 47% 4-year OS (61% transplanted, 39% nontransplanted) 24 received alloHSCT, 3 received autoHSCT |
| Vignetti et al (2007)38 GIMEMA LAL0101-B | Imatinib 800 mg daily + prednisone (induction protocol only) | 2 | 29 | First | >60 | 0% induction 2 died in CR | 100% CR 1/27 CMR | 48% (95% CI, 28-69) 1-year DFS 74% (95% CI, 54-94) 1-year OS |
| Foà et al (2011)39 GIMEMA LAL1205 | Dasatinib 70 mg twice daily + prednisone (induction protocol only) | 2 | 53 | First | ≥18 (22%> 60) | 0% induction | 100% CR 52.1% 3-log reduction in BCR-ABL by day 85 | 69% (95% 61-79) 20-month OS 51% (95% CI, 44-59) 20-month DFS |
| Martinelli et al (2017)40 GIMEMA LAL1811 NCT01641107 | Ponatinib 45 mg daily + prednisone (induction protocol only) | 2 | 42 | First | >60 or unfit | 0% induction 1 death in follow-up ponatinib | 95.5% CR 45% CMR at 24 weeks | 87.5% (95% CI, 76.5%-99.9%) 1-year OS |
| Luskin et al (2019)42 DFCI IST NCT03595917 | Dasatinib 140 + asciminib (dose escalation) (induction protocol only) | 1 | 8 | First | >50 | 0% induction | 100% CR | Not reported |
| Foà et al (2020)43 GIMEMA LAL2116 NCT02744768 | Dasatinib 140 + prednisone Blinatumomab consolidation | 2 | 63 | First | ≥18 (median 54) | 1.6% induction (1 patient) No regimen related deaths in CR | 95% CR | With median follow-up 18 months 95% (95% CI, 90-100) OS 88% (95% CI, 80-97) DFS |
| Wieduwilt et al (2018)41 NCTN/Alliance 10701 NCT01256398 | Dasatinib 140 + dexamethasone induction CC consolidation Allo- vs autoHSCT | 2 | 64 | First | ≥18 (median 60) | 0% induction deaths | 97% CR | 43% 3-year DFS (55% allo, 43% auto, 46% chemo) 55% 3-year OS (63% ≤ 60 years, 49%> 60 years) (75% allo, 71% auto, 55% chemo) Relapse 25% allo, 43% auto, 37% chemo |
| NCTN/EA9181 NCT04530565 | TKI + prednisone induction TKI + hyper-CVAD vs TKI + blinatumomab consolidation | 3 | — | First | ≥18-75 | Results pending | Results pending | Results pending |
| SWOG 1318 NCT02143414 | Dasatinib + prednisone induction Dasatinib + blinatumomab consolidation | 2 | — | First | ≥65 | Results pending | Results pending | Results pending |
| Reference | Regimen | Phase | N | Line | Age, y | Regimen- related deaths | Response | Survival |
|---|---|---|---|---|---|---|---|---|
| Rousselot et al (2016)35 EWALL PH-01 NCT028889777 | Dasatinib 140 mg daily + low-intensity CC | 2 | 71 | First | ≥55 | 4% (3/71) induction 12% (6/71) treatment-related mortality in CR | 96% CR 65% 3-log reduction in BCR-ABL | 27% (95% CI, 17-37) 5-year EFS 36% (95% CI, 25-47) 5-year OS 7 received HSCT 75% of relapses T315I |
| Ottmann et al (2018)36 EWALL PH-02 NCT028889777 | Nilotinib 400 mg twice daily + low-intensity CC | 2 | 79 | First | ≥55 | 1% (1/79) induction 11 died in CR (6 after HSCT) | 94.4% CR | 42% 4-year EFS 47% 4-year OS (61% transplanted, 39% nontransplanted) 24 received alloHSCT, 3 received autoHSCT |
| Vignetti et al (2007)38 GIMEMA LAL0101-B | Imatinib 800 mg daily + prednisone (induction protocol only) | 2 | 29 | First | >60 | 0% induction 2 died in CR | 100% CR 1/27 CMR | 48% (95% CI, 28-69) 1-year DFS 74% (95% CI, 54-94) 1-year OS |
| Foà et al (2011)39 GIMEMA LAL1205 | Dasatinib 70 mg twice daily + prednisone (induction protocol only) | 2 | 53 | First | ≥18 (22%> 60) | 0% induction | 100% CR 52.1% 3-log reduction in BCR-ABL by day 85 | 69% (95% 61-79) 20-month OS 51% (95% CI, 44-59) 20-month DFS |
| Martinelli et al (2017)40 GIMEMA LAL1811 NCT01641107 | Ponatinib 45 mg daily + prednisone (induction protocol only) | 2 | 42 | First | >60 or unfit | 0% induction 1 death in follow-up ponatinib | 95.5% CR 45% CMR at 24 weeks | 87.5% (95% CI, 76.5%-99.9%) 1-year OS |
| Luskin et al (2019)42 DFCI IST NCT03595917 | Dasatinib 140 + asciminib (dose escalation) (induction protocol only) | 1 | 8 | First | >50 | 0% induction | 100% CR | Not reported |
| Foà et al (2020)43 GIMEMA LAL2116 NCT02744768 | Dasatinib 140 + prednisone Blinatumomab consolidation | 2 | 63 | First | ≥18 (median 54) | 1.6% induction (1 patient) No regimen related deaths in CR | 95% CR | With median follow-up 18 months 95% (95% CI, 90-100) OS 88% (95% CI, 80-97) DFS |
| Wieduwilt et al (2018)41 NCTN/Alliance 10701 NCT01256398 | Dasatinib 140 + dexamethasone induction CC consolidation Allo- vs autoHSCT | 2 | 64 | First | ≥18 (median 60) | 0% induction deaths | 97% CR | 43% 3-year DFS (55% allo, 43% auto, 46% chemo) 55% 3-year OS (63% ≤ 60 years, 49%> 60 years) (75% allo, 71% auto, 55% chemo) Relapse 25% allo, 43% auto, 37% chemo |
| NCTN/EA9181 NCT04530565 | TKI + prednisone induction TKI + hyper-CVAD vs TKI + blinatumomab consolidation | 3 | — | First | ≥18-75 | Results pending | Results pending | Results pending |
| SWOG 1318 NCT02143414 | Dasatinib + prednisone induction Dasatinib + blinatumomab consolidation | 2 | — | First | ≥65 | Results pending | Results pending | Results pending |
Results at most recent publication.
CMR, complete molecular response; DFS, disease-free survival; EFS, event-free survival.
Curtain call on chemotherapy for Ph± ALL?
The Italian Gruppo Italiano Malattie EMatologiche dell’Adulto (GIMEMA) group has pioneered a chemotherapy-free induction approach for Ph+ ALL (Table 3). Imatinib plus corticosteroids induced universal hematologic remissions, although with limited depth (only 1 of 29 achieved a complete molecular remission) and durability (median duration of hematologic response of 8 months).38 Subsequently, the more potent TKI dasatinib was combined with corticosteroids, with more patients achieving deep molecular remissions (52.1% achieved BCR-ABL level <10−3 by day 85).39,40 The original GIMEMA studies were induction-only studies, with subsequent consolidation therapy for each patient dictated by the treating physician. The US NCTN Alliance 10701 phase 2 study (NCT01256398, Table 3) tested a chemotherapy-free dasatinib plus steroid induction followed by dasatinib plus CC consolidation and then transplant (allogeneic vs autologous HSCT or chemotherapy based on availability of an human leukocyte antigen (HLA)-matched donor and fitness).41 Deep remissions were consistently obtained (97% CR, 75% ultimately achieving a complete molecular response) with 3-year OS of 55% (49% in patients aged >60 years).
Although the GRAAPH-2005 study showed that intensive CC induction was not advantageous compared with lower-intensity CC induction in the context of TKIs, the benefit of adding CC to TKI-based consolidation, particularly in patients bridging to allogeneic HSCT, is not known.
Approaches to prevent relapse in Ph± ALL
Despite improvements with TKI-based therapy, relapse remains common, with T315I-driven relapses a particular menace.35,39 Approaches to address this issue include use of ponatinib, which is active against T315I; dual ABL kinase inhibition with dasatinib and asciminib; and addition of novel agent consolidation with blinatumomab.
The GIMEMA group has extended its chemotherapy-free induction approach to ponatinib plus steroids in older adults (aged ≥60 years), with encouraging early results (NCT01641107, Table 3).40 Although toxicity appears reasonable with dose reductions (only 15/42 remained at 45 mg daily at week 24), the risk of cardiovascular toxicity with ponatinib remains a concern in older patients. The planned EWALL-03 study (NCT04688983) is randomizing patients to imatinib vs ponatinib in combination with low-intensity CC and may provide insight regarding risk/benefit ratio of later-generation TKIs. A “risk-adapted” approach using early response milestones to select which patients require escalation of therapy to more potent (and more toxic) later-generation TKIs would be attractive.
Combination ABL kinase inhibition is being explored in a phase 1 study treating newly diagnosed adults 50 years or older with Ph+ ALL with dasatinib and asciminib, a novel myristoyl binding pocket inhibitor (NCT03595917, Table 3). The hypothesis is that dual ABL inhibition may induce deeper remissions and prevent T315I relapses. Thus far, the regimen appears well tolerated, with asymptomatic amylase and lipase elevations being the most notable adverse event.42 This study is ongoing to establish tolerability and recommended dose.
The GIMEMA D-ALBA trial added dasatinib-blinatumomab consolidation to dasatinib-steroid induction with promising early results (NCT02744768, Table 3).43 The US NCTN SWOG 1318 Cohort 2 (NCT02143414) is studying a similar approach of dasatinib-steroid induction followed by blinatumomab consolidation. A study of ponatinib-steroid induction followed by blinatumomab consolidation is also planned (NCT04722848). An open question is whether blinatumomab consolidation should be applied to all patients or used in a risk-adapted manner. Frequency of central nervous system (CNS) relapse will also need to be monitored over time in patients treated entirely with TKIs and novel agents (with only intrathecal (IT) chemotherapy administered to prevent CNS relapse).
Other active agents in ALL, including IO and venetoclax, also require evaluation as part of treatment of Ph+ ALL. The Alliance 041703 is planning to add an arm for Ph+ patients testing an IO plus ponatinib induction.
The US NCTN is currently accruing to EA9181 (NCT04530565), a phase 3 study of patients up to age 70 years who receive chemotherapy-free induction of TKI plus steroids and then are randomized to TKI (dasatinib or ponatinib) plus hyper-cyclophosphamide, vincristine, doxorubicin, dexamethasone (CVAD) vs TKI plus blinatumomab consolidation to compare CC vs novel agent consolidation. Eligible patients undergo transplantation when MRD negative, and all patients receive high-dose methotrexate for CNS prophylaxis.
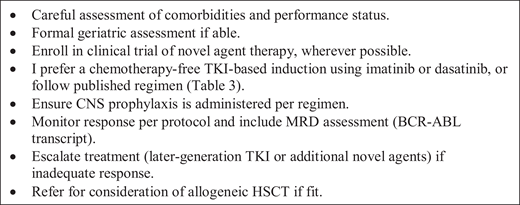
CASE 2 (continued)
The patient was treated with dasatinib and asciminib on a clinical trial. She tolerated therapy well initially but had an inadequate response after 3 cycles of therapy (CR but MRD+ by flow cytometry, BCR/ABL 6.3% IS). She required multiple dasatinib dose reductions due to recurrent pleural effusions. She was transitioned to ponatinib 30 mg daily and continues in remission (BCR-ABL p210 transcript undetectable) now 2 years from diagnosis. (See Figure 2 for approach to Ph– ALL in older adults.)
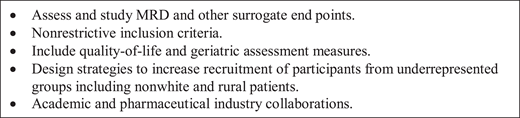
Additional issues in advancing care for older adults with ALL
The outlook for older adults diagnosed with ALL is improving rapidly. Additional issues facing the field are summarized in Figure 3.
Curability of older adults
Although survival is poor among older adults treated with CC, a few fit older patients may tolerate and be cured by CC regimens.5,11,12,44,45 In contrast, there is no evidence yet that novel agent approaches are curative, although they may induce durable MRD-negative remissions. Patients responding to novel approaches may become eligible for curative-potential allogeneic HSCT, but the role of HSCT is not clear and has not been confirmed to be superior to CC for older adults with Ph– ALL in first CR in the CC era.46 The Alliance/CALGB 10701 study has attempted to address this question for Ph+ ALL by assigning adult patients (aged 18-69 years) to reduced intensity conditioning (RIC) allogeneic HSCT vs autologous HSCT based on availability of a fully matched donor (Table 3).41 Although 3-year OS was similar between those receiving allogeneic HSCT and other consolidation approaches, patients assigned to the allogeneic approach were less likely to relapse.
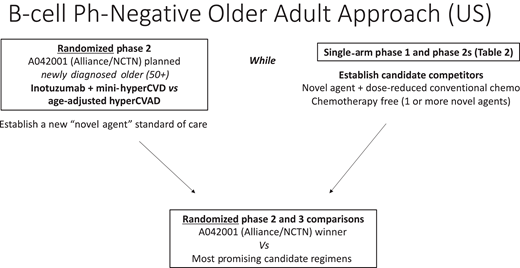
Need for randomized comparison
Results of novel agent–based regimens tested in nonrandomized studies are extremely encouraging, with strong evidence for superiority compared with historical CC regimens based on high response rates and low toxicity. The next step will be to formally compare a novel and a “standard” CC approach in Ph– ALL, and thus the NCTN is designing a randomized phase 2 study of IO plus mini-hyper-CVD (the novel regimen with the most experience to date) vs age-adjusted hyper-CVAD (Alliance 042001). The objective of this trial will be to establish a novel agent–based benchmark regimen to which other novel agent regimens can be subsequently compared (Figure 4).
Surrogate end points and risk-adapted approaches
Early response end points (such as MRD negativity) should be studied to confirm validity as surrogates for survival in older adults. This could facilitate rapid completion of trials as well as development of risk-adapted approaches.
Equity
Novel agents are expensive and likely to increase disparities between resourced and underresourced settings. Advocacy for improved access is needed.
Representative enrollment and geriatric assessment
Almost every older adult has a medical problem other than ALL. Trial eligibility should be designed to allow representative enrollment. Unnecessarily restrictive inclusion criteria that exclude patients based on advanced age, mildly compromised organ function, or “clinically insignificant” concurrent malignancies should be avoided. Geriatric assessment (GA) should be routinely incorporated into ALL trials of older adults (with financial support to ensure completion). GA has been shown to be feasible in cooperative group cancer trials, including in an Alliance trial for acute myeloid leukemia.47,48 The phase 2 NCTN trial in development plans to incorporate GA into its study design.
Quality-of-life assessment
Quality-of-life end points should be given importance. Incremental improvements in efficacy may not be “worth it” to an older adult if it is associated with significant toxicity and treatment complexity. Similarly, new regimens with equivalent responses but better tolerability may warrant further development.
Cooperation to clobber the conventional approach
By far the biggest challenge in adult ALL will be to efficiently design and conduct logical, sequential studies to answer key questions and make sure patient care “keeps up” with scientific advances. In a rare disease, this is no small task. Trials will need to be developed collaboratively, opened widely with equity considered, and conducted efficiently so that questions can be iteratively asked and answered for the betterment of patients. In the United States, a NCTN working group involving representatives from Alliance, ECOG, and SWOG has formed to coordinate efforts.
Conclusion
An older adult diagnosed with ALL in 2021 has more promising treatment options than an adult diagnosed even 5 years ago. The first task is to expeditiously replace the unacceptable traditional CC approaches with novel approaches via practice changing clinical trials. Then we must work to further define the optimal treatment for all patients considering individual (age, comorbidities, and frailty) and disease (immunophenotype, genetics, response milestones) features and personal preferences.
Conflict-of-interest disclosure
Marlise R. Luskin: discloses no relevant conflict of interest.
Off-label drug use
Marlise R. Luskin: only clinical trials discussed.
