
Learning Objectives
Review evidence for efficacy of prophylactic inferior vena cava filters (IVCFs) in trauma patients in preventing pulmonary embolism (PE)
Review evidence for efficacy of prophylactic IVCFs in trauma patients in preventing mortality
Clinical case
A 25-year-old man with no significant medical history presents to the emergency department after a motor vehicle collision. He sustained multiple fractures (injury severity score of 27). He is deemed to be high risk for bleeding with anticoagulant prophylaxis. A pneumatic compression device was placed on the lower extremities, and the surgeon on duty would like to discuss placing a prophylactic inferior vena cava filter for primary thromboprophylaxis.
pIVCFs in trauma patients
Venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common but potentially life-threatening complication of major trauma. Without appropriate thromboprophylaxis for trauma patients, the incidence of DVT and PE is as high as 18% and 11%, respectively.1 Importantly, 37% of symptomatic PE occur early after trauma, often within the first 4 days. Although fatal PE is uncommon (0.4-4.2%), 12% of deaths in trauma patients can be attributed to PE.1 Thus, PE is consistently identified as a preventable cause of death and target for improved prevention strategies. The 2019 American Society of Hematology guidelines for prevention of VTE in surgical hospitalized patients recommend routine anticoagulant prophylaxis with either low-dose unfractionated heparin or low-molecular-weight heparin over no prophylaxis in major trauma patients at low to moderate risk of bleeding.2 However, because of high bleeding risk, anticoagulant thromboprophylaxis is often contraindicated, and mechanical prophylaxis with graduated compressions stockings, intermittent pneumatic compression devices, or prophylactic inferior vena cava filters (pIVCFs) are considered. With the advent of retrievable IVCFs, utilization of these devices for primary VTE prophylaxis has expanded disproportionately to the data supporting their use and guideline recommendations.3
To examine current best evidence of pIVCFs on PE and mortality risk in trauma patients, we conducted a PubMed search of articles published from inception to 31 May 2020 using the following search terms: (trauma[MeSH Terms]) AND (“vena cava filters”[MeSH Terms]). To evaluate the highest quality data available, PubMed “Article Type” filters were applied for clinical trial, meta-analysis, randomized controlled trial, review, and systematic reviews. No language filters were used. All articles identified were reviewed for the following inclusion criteria: (1) meta-analysis, randomized controlled trial (RCT), or observational study, (2) trauma patients comprised at least a portion of the study population, (3) at least a portion of IVCFs used were for prophylaxis (before any known VTE), (4) a statistical comparison between patients with and without pIVCFs in trauma patients was reported, and (5) clinical outcomes for PE or mortality were provided. To broaden our search, references of review articles and known guidelines on the topic were screened for studies not previously identified. Both authors screened selected articles first by titles, then by abstracts, and subsequently by full-text articles. Disagreement between authors was resolved by consensus. Our systematic search identified a total of 10 articles: 3 clinical trials, 4 study-level meta-analyses, and 3 additional observational studies not included in these meta-analyses (Table 1; Figure 1).1,3-12 Data from all identified studies were extracted by both authors.
Clinical trials, systematic review and meta-analyses, and observational studies
| Study | Study design | Studies | Population | Intervention | Comparator | Efficacy outcomes | Safety outcomes |
|---|---|---|---|---|---|---|---|
| Clinical trials | |||||||
| Fullen et al 19734 | Quasi-RCT | N/A | Traumatic fracture of the proximal femur without VTE | Permanent IVCF (n = 41) | No IVCF (n = 59) | PE: 4 (10%) in IVCF group vs 19 (32%) in non-IVCF group Mortality: 4 (10%) in IVCF group vs 14 (24%) in non-IVCF group | IVCF complications: none reported in either group |
| Rajasekhar et al 20115 | Randomized pilot feasibility study | N/A | High-risk trauma patient without VTE | Retrievable IVCF and anticoagulant prophylaxis (n = 18) | Standard anticoagulant VTE prophylaxis (n = 16) | PE: 0 in IVCF group vs 1 in non-IVCF group | DVT: 1 in IVCF group vs 0 in non-IVCF group |
| Mortality: 1 in IVCF group vs 0 in non-IVCF group | IVCF retrieval: 0% at 3 mo; 15% at 6 mo | ||||||
| Ho et al 20191 | RCT | N/A | High-risk trauma patient (ISS > 15) without VTE and contraindication to AC | Retrievable IVCF (n = 122) | No IVCF (n = 118) | 90-d composite symptomatic PE or mortality: 17 (13.9%) in IVCF group vs 17 (14.4%) in non-IVCF group (HR 0.99; 95% CI 0.51-1.94; P = .98) | Symptomatic PE (after 7 d with continued contraindication to AC): 0 in IVCF group vs 5 in non-IVCF group (RR 0, 95% CI 0.00-0.55) |
| Mortality: 16 (13.1%) of IVCF group vs 11 (9.3%) of non-IVCF group (RR 1.41; 95% CI 0.69-2.87) | IVCF complications (at time of filter retrieval): 15% | ||||||
| 90-d IVCF retrieval: 71 of 108 (66%) | |||||||
| Systematic reviews and meta-analyses | |||||||
| Rajasekhar et al 20113 | Systematic review and meta-analysis | 7 observational cohort studies | High-risk trauma patient without VTE | IVCF (n = 428) (6 studies with permanent IVCFs, 1 not reported) and anticoagulant prophylaxis (in 5 studies) | No IVCF (n = 1472) and anticoagulant prophylaxis (in 5 studies) | PE: 4 of 428 (0.9%) in IVCF group vs 76 of 1472 (5%) in non-IVCF group (OR 0.21; 95% CI 0.09-0.49) | DVT*: 17 of 94 (18%) in IVCF group vs 18 of 138 (13%) in non-IVCF group (OR 1.6; 95% CI 0.76-3.37) |
| Singh et al 20136 | Systematic review and meta-analysis | 8 controlled studies: 1 pilot feasibility, 7 observational; 2 excluded from meta-analysis | Mixed trauma patient | IVCF (2 permanent IVCF; 6 not reported) (n = 432) | No IVCF (i.e. mechanical ± anticoagulant prophylaxis) (n = 4160) | PE*: 2 of 334 (0.5%) in IVCF group vs 48 of 730 (6.5%) in non-IVCF group (RR 0.20; 95% CI 0.06-0.70) | Fatal PE*: 0 of 163 (0%) in IVCF group vs 20 of 407 (4.9%) in non-IVCF group (RR 0.09; 95% CI 0.01-0.81) |
| Mortality*: 21 of 166 (12.6%) in IVCF group vs 60 of 312 (19.2%) in non-IVCF group (RR 0.7; 95% CI 0.4-1.23) | DVT*: 18 of 112 (16%) in IVCF group vs 18 of 154 (11.7%) in non-IVCF group (RR 1.76; 95% CI 0.49-6.18; P = .38) | ||||||
| Filter complication* 1.0%-5.7% | |||||||
| Haut et al 20147 | Systematic review and meta-analysis | 8 controlled studies: 1 pilot feasibility, 7 observational – 2 excluded from meta-analysis | Mixed trauma patient | IVCF and standard VTE prophylaxis (n = 334) | Standard VTE prophylaxis (n = 730) | PE: 2 (0.5%) in IVCF group vs 48 (6.5%) in non-IVCF group (RR 0.20; 95% CI 0.06-0.70) | Fatal PE*: 0 in IVCF group vs 20 of 407 (4.9%) in non-IVCF group (RR 0.09; 95% CI 0.01-0.81) |
| Mortality*: RR 0.70 [95% CI 0.4-1.23] | DVT*: RR 1.76; 95% CI 0.50-6.19, P = .38) | ||||||
| Shariff et al 20208 | Systematic review and meta-analysis | 10 controlled studies: 2 RCTs, 8 observational studies | High-risk trauma patients (ISS > 15 or trauma delaying initiation of VTE prophylaxis) | IVCF (n = 573) | Standard VTE prophylaxis (n = 1717) | Symptomatic PE: 5 (0.87%) in IVCF group vs 90 (5.2%) in non-IVCF group (RR 0.27; 95% CI 0.12-0.58; P < 0.05) | Fatal PE*: 0 in IVCF group vs 23 of 619 (3.7%) in non-IVCF group (RR 0.29; 95% CI 0.08-1.10; P = .07) |
| Observational studies | |||||||
| Batty et al 20129 | Prospective cohort study with concurrent controls | N/A | High-risk trauma patient without VTE | IVCF (n = 511) | No IVCF (n = 5833) | PE: OR 0.28; 95% CI 0.088-0.890; P = .031 | NR |
| Hemmila et al 201510 | Retrospective cohort study | N/A | High-risk trauma patient without VTE | IVCF (n = 803) | No IVCF (n = 39456) | PE: 9 (1.1%) in IVCF group vs 187 (0.5%) in non-IVCF group (P = .01) | DVT: 54 (6.7%) in IVCF group vs 483 (1.2%) in non-IVCF group (P < .001) |
| Mortality: 42 (5.2%) in IVCF group vs 1369 (3.5%) in non-IVCF group (P = .01) | |||||||
| Sarosiek et al 201711 | Retrospective cohort study | N/A | High-risk trauma patient without VTE | IVCF (n = 451) | No IVCF (n = 1343) | Mortality: IVCF group with higher mortality than non-IVCF group (P = .14) | NR |
| Study | Study design | Studies | Population | Intervention | Comparator | Efficacy outcomes | Safety outcomes |
|---|---|---|---|---|---|---|---|
| Clinical trials | |||||||
| Fullen et al 19734 | Quasi-RCT | N/A | Traumatic fracture of the proximal femur without VTE | Permanent IVCF (n = 41) | No IVCF (n = 59) | PE: 4 (10%) in IVCF group vs 19 (32%) in non-IVCF group Mortality: 4 (10%) in IVCF group vs 14 (24%) in non-IVCF group | IVCF complications: none reported in either group |
| Rajasekhar et al 20115 | Randomized pilot feasibility study | N/A | High-risk trauma patient without VTE | Retrievable IVCF and anticoagulant prophylaxis (n = 18) | Standard anticoagulant VTE prophylaxis (n = 16) | PE: 0 in IVCF group vs 1 in non-IVCF group | DVT: 1 in IVCF group vs 0 in non-IVCF group |
| Mortality: 1 in IVCF group vs 0 in non-IVCF group | IVCF retrieval: 0% at 3 mo; 15% at 6 mo | ||||||
| Ho et al 20191 | RCT | N/A | High-risk trauma patient (ISS > 15) without VTE and contraindication to AC | Retrievable IVCF (n = 122) | No IVCF (n = 118) | 90-d composite symptomatic PE or mortality: 17 (13.9%) in IVCF group vs 17 (14.4%) in non-IVCF group (HR 0.99; 95% CI 0.51-1.94; P = .98) | Symptomatic PE (after 7 d with continued contraindication to AC): 0 in IVCF group vs 5 in non-IVCF group (RR 0, 95% CI 0.00-0.55) |
| Mortality: 16 (13.1%) of IVCF group vs 11 (9.3%) of non-IVCF group (RR 1.41; 95% CI 0.69-2.87) | IVCF complications (at time of filter retrieval): 15% | ||||||
| 90-d IVCF retrieval: 71 of 108 (66%) | |||||||
| Systematic reviews and meta-analyses | |||||||
| Rajasekhar et al 20113 | Systematic review and meta-analysis | 7 observational cohort studies | High-risk trauma patient without VTE | IVCF (n = 428) (6 studies with permanent IVCFs, 1 not reported) and anticoagulant prophylaxis (in 5 studies) | No IVCF (n = 1472) and anticoagulant prophylaxis (in 5 studies) | PE: 4 of 428 (0.9%) in IVCF group vs 76 of 1472 (5%) in non-IVCF group (OR 0.21; 95% CI 0.09-0.49) | DVT*: 17 of 94 (18%) in IVCF group vs 18 of 138 (13%) in non-IVCF group (OR 1.6; 95% CI 0.76-3.37) |
| Singh et al 20136 | Systematic review and meta-analysis | 8 controlled studies: 1 pilot feasibility, 7 observational; 2 excluded from meta-analysis | Mixed trauma patient | IVCF (2 permanent IVCF; 6 not reported) (n = 432) | No IVCF (i.e. mechanical ± anticoagulant prophylaxis) (n = 4160) | PE*: 2 of 334 (0.5%) in IVCF group vs 48 of 730 (6.5%) in non-IVCF group (RR 0.20; 95% CI 0.06-0.70) | Fatal PE*: 0 of 163 (0%) in IVCF group vs 20 of 407 (4.9%) in non-IVCF group (RR 0.09; 95% CI 0.01-0.81) |
| Mortality*: 21 of 166 (12.6%) in IVCF group vs 60 of 312 (19.2%) in non-IVCF group (RR 0.7; 95% CI 0.4-1.23) | DVT*: 18 of 112 (16%) in IVCF group vs 18 of 154 (11.7%) in non-IVCF group (RR 1.76; 95% CI 0.49-6.18; P = .38) | ||||||
| Filter complication* 1.0%-5.7% | |||||||
| Haut et al 20147 | Systematic review and meta-analysis | 8 controlled studies: 1 pilot feasibility, 7 observational – 2 excluded from meta-analysis | Mixed trauma patient | IVCF and standard VTE prophylaxis (n = 334) | Standard VTE prophylaxis (n = 730) | PE: 2 (0.5%) in IVCF group vs 48 (6.5%) in non-IVCF group (RR 0.20; 95% CI 0.06-0.70) | Fatal PE*: 0 in IVCF group vs 20 of 407 (4.9%) in non-IVCF group (RR 0.09; 95% CI 0.01-0.81) |
| Mortality*: RR 0.70 [95% CI 0.4-1.23] | DVT*: RR 1.76; 95% CI 0.50-6.19, P = .38) | ||||||
| Shariff et al 20208 | Systematic review and meta-analysis | 10 controlled studies: 2 RCTs, 8 observational studies | High-risk trauma patients (ISS > 15 or trauma delaying initiation of VTE prophylaxis) | IVCF (n = 573) | Standard VTE prophylaxis (n = 1717) | Symptomatic PE: 5 (0.87%) in IVCF group vs 90 (5.2%) in non-IVCF group (RR 0.27; 95% CI 0.12-0.58; P < 0.05) | Fatal PE*: 0 in IVCF group vs 23 of 619 (3.7%) in non-IVCF group (RR 0.29; 95% CI 0.08-1.10; P = .07) |
| Observational studies | |||||||
| Batty et al 20129 | Prospective cohort study with concurrent controls | N/A | High-risk trauma patient without VTE | IVCF (n = 511) | No IVCF (n = 5833) | PE: OR 0.28; 95% CI 0.088-0.890; P = .031 | NR |
| Hemmila et al 201510 | Retrospective cohort study | N/A | High-risk trauma patient without VTE | IVCF (n = 803) | No IVCF (n = 39456) | PE: 9 (1.1%) in IVCF group vs 187 (0.5%) in non-IVCF group (P = .01) | DVT: 54 (6.7%) in IVCF group vs 483 (1.2%) in non-IVCF group (P < .001) |
| Mortality: 42 (5.2%) in IVCF group vs 1369 (3.5%) in non-IVCF group (P = .01) | |||||||
| Sarosiek et al 201711 | Retrospective cohort study | N/A | High-risk trauma patient without VTE | IVCF (n = 451) | No IVCF (n = 1343) | Mortality: IVCF group with higher mortality than non-IVCF group (P = .14) | NR |
AC, anticoagulation; CI, confidence interval; HR, hazard ratio; ISS, Injury Severity Score; N/A, not applicable; NR, not reported; OR, odds ratio; RR, relative risk.
Outcome not reported in all studies.
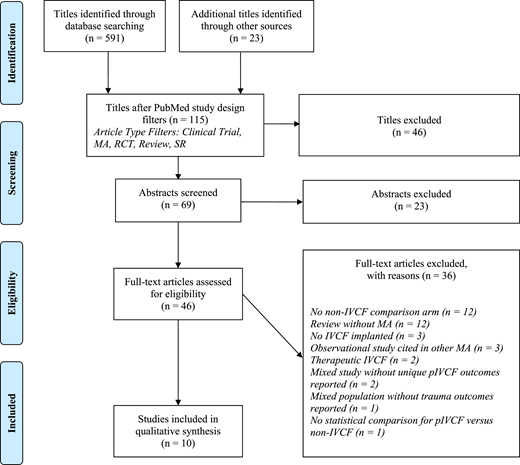
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. PRISMA methodology: Moher et al.12 MA, meta-analysis; SR, systematic review.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. PRISMA methodology: Moher et al.12 MA, meta-analysis; SR, systematic review.
Does the literature support IVCFs in trauma patients for primary VTE prophylaxis? Numerous nonrandomized cohort studies have evaluated the efficacy of pIVCFs in trauma patients. These studies have inherent limitations including lack of a control group not receiving an IVCF, variance in reporting details of patient baseline characteristics, different definitions for high-risk trauma patients, lack of documented or standardized contemporary anticoagulant prophylaxis, different screening patterns for VTE, and limited follow-up for clinical outcomes after hospital discharge. Only 3 clinical trials have investigated the role of pIVCFs in trauma patients. In 1973, Fullen et al4 randomized 129 patients with traumatic femoral fractures to pIVCF vs. no IVCF. Significant reductions in PE and mortality were reported, driven primarily by a reduction in fatal PE. This study was limited by absence of anticoagulant prophylaxis in any group, high crossover from the filter to nonfilter group, and the inclusion of possible PE without radiologic confirmation of diagnosis. In 2011, Rajasekhar et al5 performed a prospective pilot feasibility study randomizing high-risk trauma patients to pIVCF vs no IVCF. All patients also received anticoagulant prophylaxis. At 6 months, 1 PE occurred in the non-IVCF arm and 1 death in the IVCF arm. This study was not powered to detect differences in clinical outcomes but showed feasibility of conducting a larger scale study. In 2019, Ho et al1 randomized 240 major trauma patients with contraindications to anticoagulation to an IVCF, placed within 72 hours of admission, vs no IVCF. After 90 days, early IVCF placement was not associated with a lower risk of the composite end point (symptomatic PE) and death. Within 7 days of injury, 67% had started anticoagulant prophylaxis. Of those with ongoing contraindications to prophylactic anticoagulation, symptomatic PE developed in none in the IVCF group and 5 in the non-IVCF group, including 1 fatal PE. Notably survivor bias could have affected this subgroup analysis.
Numerous reviews discuss primary VTE prophylaxis with IVCFs in trauma patients, but only 4 met our inclusion criteria.3,6-8 One study-level meta-analysis by Rajasekhar et al3 critically appraised results from comparative observational studies and found a lower risk for PE but no difference in DVT or mortality in trauma patients treated with pIVCFs compared with a non-IVCF group. However, significant heterogeneity among studies limited firm conclusions. A 2013 meta-analysis by Singh et al6 included the 2011 pilot RCT and 5 observational studies. All included studies compared an IVCF group in addition to standard VTE prophylaxis against standard prophylaxis alone, although there was variance in types of outcomes reported. Notably, the definition of standard prophylaxis varied between trials, ranging from either anticoagulant or mechanical prophylaxis alone or combined prophylaxis. All studies were judged to have a moderate to high risk of bias. A precise and consistent reduction in PE with IVCFs was reported in all studies without evidence of statistical heterogeneity. IVCFs were found to be protective against fatal PE, although sensitivity analysis did not reveal robustness in this outcome. Mortality and DVT were not different between groups. Retrieval rates were not consistently reported. A subsequent 2014 meta-analysis arrived at the same conclusions based on the same body of evidence.7 In this meta-analysis, Haut et al estimated 109 to 962 trauma patients (assuming a baseline PE risk of 0.13-1.15%) would need to receive an IVCF to prevent 1 PE. With a case fatality rate of 10%, 1099 patients would need to receive a pIVCF to prevent 1 fatal PE. The most recent meta-analysis on this topic by Shariff et al8 included the 2011 and 2019 clinical trials and 8 observational studies, all deemed to have high risk of bias, and was the only review to include the highest quality data from the large clinical trial by Ho et al.1 A lower risk of symptomatic PE without difference in fatal PE was observed in patients that received a pIVCF compared with no pIVCF. No significant heterogeneity in the pooled estimates or publication bias was present.
We found 3 additional observational studies in our systematic review that were not included in the above meta-analyses.9-11 A trauma registry study by Batty et al9 found that the presence of a pIVCF was independently associated with lower risk for PE. However, this study was limited by its retrospective nature and low incidence of PE overall compared with those without an IVCF. Sarosiek et al11 evaluated mortality outcomes in trauma patients who received an IVCF compared with propensity-matched controls without an IVCF. Placement of an IVCF did not affect short-term or long-term mortality in those that survived their initial injury after 24 hours, regardless of whether the IVCF was placed for prophylactic or therapeutic indications. Finally, analysis of a collaborative registry from 26 trauma centers by Hemmila et al10 found that pIVCFs were associated with higher rates of mortality, DVT, PE, and overall VTE, although IVCF patients had higher baseline injury severity scores compared with non-IVCF patients.
In conclusion, there is low quality evidence based on the Grading of Recommendations Assessment, Development, and Evaluation approach that prophylactic IVCF use in patients with major trauma reduces the incidence of PE in the absence of a reduction in mortality.13 Given the potential increased risk of DVT, known complications associated with these devices, low retrieval rate in the relatively young healthy trauma population, and lack of cost-effectiveness with this approach, IVCFs should not be used routinely in trauma patients for primary VTE prophylaxis.14
Correspondence
Anita Rajasekhar, University of Florida, 1600 SW Archer Rd, Gainesville, FL 32610; e-mail: anita.rajasekhar@medicine.ufl.edu.
