
Abstract
A 77-year-old man with atrial fibrillation and a CHA2DS2Vasc score of 6 for hypertension, age, diabetes, and previous stroke is brought to the emergency department with decreased level of consciousness. He is anticoagulated with rivaroxaban (a direct oral factor Xa inhibitor [FXaI]) and received his last dose about 4 hours before presentation. Urgent computed tomography of the head shows intracerebral hemorrhage. Because of his previous stroke, the patient’s family is concerned about treating the bleed with pharmacological agents that may increase the risk of stroke. What are the risks of thrombosis and mortality related to the use of prothrombin complex concentrates (PCCs) and andexanet alfa for patients with direct oral FXaI-associated major bleeding?
Learning Objectives
Summarize the evidence regarding the use of prothrombin complex concentrates and andexanet alfa for the management of direct oral factor Xa inhibitor–associated major bleeding
Calculate the rates and cumulative incidences of mortality and thrombosis related to the use of prothrombin complex concentrates and andexanet alfa for the management of direct oral factor Xa inhibitor–associated major bleeding
Discussion
Direct oral anticoagulants are widely used to prevent and treat thromboembolism, most often to reduce the risk of stroke and embolic phenomena in atrial fibrillation and for the treatment and secondary thromboprophylaxis of venous thromboembolism. Idarucizumab, a specific reversal agent for the direct oral thrombin inhibitor dabigatran, is approved for the management of major bleeding events (MBEs) or in preparation for urgent surgery. Andexanet alfa was designed as a specific reversal agent for direct and indirect FXaIs and is currently approved in the United States and Europe for the reversal of apixaban and rivaroxaban in patients with MBE on the basis of the registration study (Prospective, Open-Label Study of Andexanet Alfa in Patients Receiving a Factor Xa Inhibitor Who Have Acute Major Bleeding [ANNEXA-4]). Andexanet is a recombinant, inactive form of factor Xa that binds and sequesters the FXaI and therefore neutralizes its anticoagulant effect. However, andexanet is not widely available, and its use is associated with important cost implications for hospitals and health care systems. PCCs have been used off-label for the management of MBE in patients receiving direct oral FXaIs. Four-factor PCC (4F-PCC) contains the vitamin K–dependent coagulation factors II, VII, IX, and X, whereas the 3-factor PCC does not contain factor VII. Some centers have developed protocols with activated prothrombin complex concentrates (aPCCs) for the management of FXaI-associated MBE. aPCC contains activated factor VII and mostly inactivated factors II, IX, and X. A recent systematic review aimed to characterize the hemostatic efficacy of PCC for the management of FXaI-associated MBE.1 However, a meta-analysis of the hemostatic efficacy of PCC for this indication could not be performed, owing to the heterogeneous definitions of adequate hemostasis adopted by the included studies. Therefore, we sought to summarize the safety outcomes of these FXaI-associated MBE management strategies by providing early (in-hospital) and late (at 30-day follow-up) rates and cumulative incidences for overall mortality and thrombotic complications.
We systematically searched MEDLINE and Embase to identify articles assessing mortality and thrombotic complications associated with the use of PCC, aPCC, and andexanet for the management of FXaI-associated major bleeding. We also sought to explore the different definitions of hemostatic effectiveness used in studies assessing these different hemostatic agents for the management of MBE in patients receiving FXaI. We modified and updated a search strategy devised for the synthesis of evidence in the context of the American Society of Hematology guideline development on optimal management of anticoagulation therapy.1 We included published randomized controlled trials, prospective cohort studies, retrospective cohort studies, and case series (with at least 10 patients) designed to evaluated the safety and efficacy of PCC, aPCC, or andexanet for the management of FXaI-associated MBE. Studies of patients needing hemostatic support in preparation for emergent surgery were excluded because the objective of the review was to inform clinicians regarding the risks of death and thrombosis in patients receiving PCC, aPCC, or andexanet for FXaI-associated MBE. Title and abstract screening, full-text review, and data extraction were conducted in duplicate by 2 independent reviewers using Covidence software (Covidence, Melbourne, Australia). When appropriate, pooled rates and cumulative incidences for overall mortality and thrombosis were calculated using StatsDirect software (StatsDirect, Birkenhead, UK).
A total of 1459 citations were identified (Figure 1). After duplicate removal, 1282 references were screened. There were 146 references that underwent full-text review, and 15 were included. Of those, 13 observational studies assessed the use of PCC, 1 retrospective study examined the use of aPCC, and 1 prospective study addressed the use of andexanet in our patient population. The majority of excluded studies at the full-text review stage were abstracts, and a smaller number did not contain the appropriate patient population or report outcomes of interest or did not have the included study designs. The risk of bias of included studies was assessed according to guidance for nonrandomized studies provided in the Cochrane Handbook.2
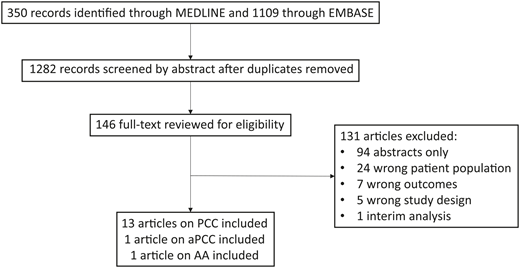
Study flow diagram. AA, andexanet alfa; aPCC, activated prothrombin complex concentrate; PCC, prothrombin complex concentrate.
Study flow diagram. AA, andexanet alfa; aPCC, activated prothrombin complex concentrate; PCC, prothrombin complex concentrate.
PCCs
Thirteen nonrandomized, unblinded studies including 521 patients evaluated the use of PCCs in the management of MBE in patients receiving an FXaI (Table 1). Four studies were prospective,3-6 and nine studies were retrospective.7-15 The majority (69%) of studies followed patients only during hospital admission.6,7,9-15 On average, the hospital admission lasted 6.6 days. Four studies had a follow-up period of 30 days.3-5,8 Most of the included patients were receiving rivaroxaban for stroke prophylaxis in atrial fibrillation. Intracranial hemorrhage was the most common reason for the administration of PCC. A minority (38%) of studies defined major bleeding per the International Society on Thrombosis and Haemostasis (ISTH) definition.16 The definition of effective hemostasis was provided in 9 studies and varied across studies, with 2 studies3,14 using the ISTH definition,17 2 studies5,15 using the definition proposed by Sarode et al,18 and 5 studies4,7-9,11 using their own definition of effective hemostasis. Most patients were judged to have achieved adequate hemostasis on the basis of various definitions of hemostatic effectiveness employed by the included studies. All studies were judged to be at high risk for bias as single-cohort studies lacking control groups.
Characteristics of the 13 included studies assessing the use of prothrombin complex concentrate in factor Xa inhibitor–associated major bleeding
| Reference | Study design | No. | Treatment | Major bleeding definition | Factor Xa inhibitor | Indication for anticoagulation | Follow-up (d) | Intracranial hemorrhage | Gastrointestinal bleeding | Other bleeding |
|---|---|---|---|---|---|---|---|---|---|---|
| Allison7 | Retrospective | 33 | 4F-PCC (35 U/kg) | Other | Apixaban = 6 | AF = 24 | 7.1 | 30 | 1 | 2 |
| Rivaroxaban = 27 | VTE = 6 | |||||||||
| Other = 3 | ||||||||||
| Arachchillage8 | Retrospective | 80 | 4F-PCC | ISTH | Apixaban = 40 | AF = 67 | 30 | 46 | 24 | 10 |
| Rivaroxaban = 40 | VTE = 12 | |||||||||
| Both = 1 | ||||||||||
| Berger9 | Retrospective | 22 | 4F-PCC (25 U/kg) | Other | Apixaban = 5 | AF = 17 | 5.9 | 22 | — | — |
| Rivaroxaban = 15 | VTE = 4 | |||||||||
| Dabigatran = 2 | Other = 3 | |||||||||
| (>1 possible per patient) | ||||||||||
| Dybdahl10 | Retrospective | 35 | 4F-PCC (50 U/kg) | Other | Apixaban = 17 | AF = 30 | 6.4 | 35 | — | — |
| Rivaroxaban = 18 | VTE = 4 | |||||||||
| Both = 1 | ||||||||||
| Grandhi11 | Retrospective | 18 | 4F-PCC | Other | Apixaban = 2 | AF = 15 | 8.4 | 18 | — | — |
| Rivaroxaban = 18 | VTE = 1 | |||||||||
| Both = 1 | ||||||||||
| Other = 1 | ||||||||||
| Harrison12 | Retrospective | 14 | 4F-PCC | Other | N/A | AF = 12 | 7.1 | 14 | — | — |
| VTE = 3 | ||||||||||
| Other = 2 | ||||||||||
| (>1 possible per patient) | ||||||||||
| Majeed3 | Prospective | 84 | 4F-PCC (25 U/kg) | ISTH | Apixaban = 39 | AF = 63 | 30 | 59 | 13 | 12 |
| Rivaroxaban = 45 | VTE = 3 | |||||||||
| Both = 18 | ||||||||||
| Müller13 | Retrospective | 74* | 4F-PCC | N/A | Apixaban = 5 | AF = 48 | 4.9 | 45 | 14 | 14 |
| Rivaroxaban = 67 | VTE = 13 | |||||||||
| Edoxaban = 1 | Other = 13 | |||||||||
| Dabigatran = 1 | ||||||||||
| Schenk4 | Prospective | 13 | 4F-PCC (25 U/kg) | N/A | Rivaroxaban = 13 | N/A | 30 | 10 | 1 | 2 |
| Schulman5 | Prospective | 66 | 4F-PCC (2000 U) | ISTH | Apixaban = 29 | AF = 54 | 30 | 36 | 16 | 14 |
| Rivaroxaban = 37 | VTE = 8 | |||||||||
| Both = 2 | ||||||||||
| Other = 1 | ||||||||||
| Sheikh-Taha14 | Retrospective | 29 | 4F-PCC (50 U/kg) | ISTH | Apixaban = 13 | AF = 23 | 5.9 | 21 | 4 | 4 |
| Rivaroxaban = 16 | VTE = 5 | |||||||||
| Other = 1 | ||||||||||
| Smith15 | Retrospective | 31 | 4F-PCC (25-50 U/kg) | Other | Apixaban = 17 | AF = 28 | 7.2 | 18 | 1 | 12 |
| Rivaroxaban = 14 | VTE = 3 | |||||||||
| Testa6 | Prospective | 22 | PCC | ISTH | Apixaban = 6 | N/A | 3 | 20 | 2 | 0 |
| Rivaroxaban = 16 |
| Reference | Study design | No. | Treatment | Major bleeding definition | Factor Xa inhibitor | Indication for anticoagulation | Follow-up (d) | Intracranial hemorrhage | Gastrointestinal bleeding | Other bleeding |
|---|---|---|---|---|---|---|---|---|---|---|
| Allison7 | Retrospective | 33 | 4F-PCC (35 U/kg) | Other | Apixaban = 6 | AF = 24 | 7.1 | 30 | 1 | 2 |
| Rivaroxaban = 27 | VTE = 6 | |||||||||
| Other = 3 | ||||||||||
| Arachchillage8 | Retrospective | 80 | 4F-PCC | ISTH | Apixaban = 40 | AF = 67 | 30 | 46 | 24 | 10 |
| Rivaroxaban = 40 | VTE = 12 | |||||||||
| Both = 1 | ||||||||||
| Berger9 | Retrospective | 22 | 4F-PCC (25 U/kg) | Other | Apixaban = 5 | AF = 17 | 5.9 | 22 | — | — |
| Rivaroxaban = 15 | VTE = 4 | |||||||||
| Dabigatran = 2 | Other = 3 | |||||||||
| (>1 possible per patient) | ||||||||||
| Dybdahl10 | Retrospective | 35 | 4F-PCC (50 U/kg) | Other | Apixaban = 17 | AF = 30 | 6.4 | 35 | — | — |
| Rivaroxaban = 18 | VTE = 4 | |||||||||
| Both = 1 | ||||||||||
| Grandhi11 | Retrospective | 18 | 4F-PCC | Other | Apixaban = 2 | AF = 15 | 8.4 | 18 | — | — |
| Rivaroxaban = 18 | VTE = 1 | |||||||||
| Both = 1 | ||||||||||
| Other = 1 | ||||||||||
| Harrison12 | Retrospective | 14 | 4F-PCC | Other | N/A | AF = 12 | 7.1 | 14 | — | — |
| VTE = 3 | ||||||||||
| Other = 2 | ||||||||||
| (>1 possible per patient) | ||||||||||
| Majeed3 | Prospective | 84 | 4F-PCC (25 U/kg) | ISTH | Apixaban = 39 | AF = 63 | 30 | 59 | 13 | 12 |
| Rivaroxaban = 45 | VTE = 3 | |||||||||
| Both = 18 | ||||||||||
| Müller13 | Retrospective | 74* | 4F-PCC | N/A | Apixaban = 5 | AF = 48 | 4.9 | 45 | 14 | 14 |
| Rivaroxaban = 67 | VTE = 13 | |||||||||
| Edoxaban = 1 | Other = 13 | |||||||||
| Dabigatran = 1 | ||||||||||
| Schenk4 | Prospective | 13 | 4F-PCC (25 U/kg) | N/A | Rivaroxaban = 13 | N/A | 30 | 10 | 1 | 2 |
| Schulman5 | Prospective | 66 | 4F-PCC (2000 U) | ISTH | Apixaban = 29 | AF = 54 | 30 | 36 | 16 | 14 |
| Rivaroxaban = 37 | VTE = 8 | |||||||||
| Both = 2 | ||||||||||
| Other = 1 | ||||||||||
| Sheikh-Taha14 | Retrospective | 29 | 4F-PCC (50 U/kg) | ISTH | Apixaban = 13 | AF = 23 | 5.9 | 21 | 4 | 4 |
| Rivaroxaban = 16 | VTE = 5 | |||||||||
| Other = 1 | ||||||||||
| Smith15 | Retrospective | 31 | 4F-PCC (25-50 U/kg) | Other | Apixaban = 17 | AF = 28 | 7.2 | 18 | 1 | 12 |
| Rivaroxaban = 14 | VTE = 3 | |||||||||
| Testa6 | Prospective | 22 | PCC | ISTH | Apixaban = 6 | N/A | 3 | 20 | 2 | 0 |
| Rivaroxaban = 16 |
4F, four-factor; AF, atrial fibrillation; ISTH, International Society on Thrombosis and Haemostasis; N/A, not available; PCC, prothrombin complex concentrate; VTE, venous thromboembolism .
93% of patients received PCCs for major bleeding.
Using a random effects model, the pooled in-hospital overall mortality rate was 3.4 (95% confidence interval [CI], 2.5-4.3; I2 = 2.7%) per 100 person-days, and the pooled in-hospital cumulative overall mortality was 18% (95% CI, 14% to 23%; I2 = 2.6%) (Table 2). The pooled in-hospital thrombosis rate was 0.6 (95% CI, 0.2-1.1; I2 = 4.8%) per 100 person-days, and the pooled in-hospital cumulative incidence of thrombotic events was 3% (95% CI, 1% to 7%; I2 = 0%). The pooled 30-day overall mortality rate was 1.0 (95% CI, 0.6-1.6; I2 = 69.9%) per 100 person-days, and the pooled 30-day cumulative overall mortality was 26% (95% CI, 16% to 38%; I2 = 69.6%) (Table 3). The pooled 30-day thrombotic complication rate was 0.2 (95% CI, 0.1-0.4; I2 = 0%) per 100 person-days, and the pooled 30-day cumulative incidence of thrombotic events was 6% (95% CI, 3% to 9%; I2 = 13.4%).
In-hospital mortality and thrombotic complications in patients treated with prothrombin complex concentrate for a factor Xa inhibitor–associated major bleeding event
| Reference | Overall in-hospital mortality, n | Overall in-hospital cumulative mortality, % | Overall in-hospital mortality rate (per 100 person-days) | In-hospital thrombotic events, n | In-hospital thrombotic events cumulative incidence, % | In-hospital thrombotic event rate (per 100 person-days) | Hemostatic adequacy*, n (%) |
|---|---|---|---|---|---|---|---|
| Allison7 | 5 | 15% | 2.5 | 0 | 0 | 0 | 26 (84%) |
| Berger9 | 4 | 18% | 3.8 | 2 | 9% | 1.9 | 17 (94%) |
| Dybdahl10 | 8 | 23% | 4.0 | 1 | 3% | 0.5 | N/A |
| Grandhi11 | 6 | 33% | 4.8 | 1 | 6% | 0.8 | 17 (94%) |
| Harrison12 | 2 | 14% | 2.2 | 0 | 0 | 0 | 13 (93%) |
| Müller13 | 7 | 9% | 2.0 | N/A | N/A | N/A | N/A |
| Sheikh-Taha14 | 6 | 21% | 3.9 | 1 | 3% | 0.7 | 21 (72%) |
| Smith15 | 5 | 16% | 2.4 | 0 | 0 | 0 | 25 (81%) |
| Testa6 | 5 | 23% | 8.5 | N/A | N/A | N/A | N/A |
| Reference | Overall in-hospital mortality, n | Overall in-hospital cumulative mortality, % | Overall in-hospital mortality rate (per 100 person-days) | In-hospital thrombotic events, n | In-hospital thrombotic events cumulative incidence, % | In-hospital thrombotic event rate (per 100 person-days) | Hemostatic adequacy*, n (%) |
|---|---|---|---|---|---|---|---|
| Allison7 | 5 | 15% | 2.5 | 0 | 0 | 0 | 26 (84%) |
| Berger9 | 4 | 18% | 3.8 | 2 | 9% | 1.9 | 17 (94%) |
| Dybdahl10 | 8 | 23% | 4.0 | 1 | 3% | 0.5 | N/A |
| Grandhi11 | 6 | 33% | 4.8 | 1 | 6% | 0.8 | 17 (94%) |
| Harrison12 | 2 | 14% | 2.2 | 0 | 0 | 0 | 13 (93%) |
| Müller13 | 7 | 9% | 2.0 | N/A | N/A | N/A | N/A |
| Sheikh-Taha14 | 6 | 21% | 3.9 | 1 | 3% | 0.7 | 21 (72%) |
| Smith15 | 5 | 16% | 2.4 | 0 | 0 | 0 | 25 (81%) |
| Testa6 | 5 | 23% | 8.5 | N/A | N/A | N/A | N/A |
N/A, not available.
Based on evaluable patients, which may be a smaller sample than the total sample.
Thirty-day mortality and thrombotic complications in patients treated with prothrombin complex concentrate for a factor Xa inhibitor–associated major bleeding event
| Reference | Overall 30-d mortality, n | Overall 30-d cumulative mortality, % | Overall 30-d mortality rate (per 100 person-days) | 30-d thrombotic events, n | 30-d thrombotic events cumulative incidence, % | 30-d thrombotic event rate (per 100 person-days) | Hemostatic adequacy, n (%) |
|---|---|---|---|---|---|---|---|
| Arachchillage8 | 27 | 34% | 1.4 | 3 | 3.8% | 0.2 | 59 (74%) |
| Majeed3 | 27 | 32% | 1.3 | 3 | 3.6% | 0.1 | 58 (69%) |
| Schenk4 | 3 | 23% | 0.9 | 2 | 15.4% | 0.6 | 10 (78%) |
| Schulman5 | 9 | 14% | 0.5 | 5 | 7.6% | 0.3 | 43 (65%) |
| Reference | Overall 30-d mortality, n | Overall 30-d cumulative mortality, % | Overall 30-d mortality rate (per 100 person-days) | 30-d thrombotic events, n | 30-d thrombotic events cumulative incidence, % | 30-d thrombotic event rate (per 100 person-days) | Hemostatic adequacy, n (%) |
|---|---|---|---|---|---|---|---|
| Arachchillage8 | 27 | 34% | 1.4 | 3 | 3.8% | 0.2 | 59 (74%) |
| Majeed3 | 27 | 32% | 1.3 | 3 | 3.6% | 0.1 | 58 (69%) |
| Schenk4 | 3 | 23% | 0.9 | 2 | 15.4% | 0.6 | 10 (78%) |
| Schulman5 | 9 | 14% | 0.5 | 5 | 7.6% | 0.3 | 43 (65%) |
Activated prothrombin complex concentrate
One retrospective chart review evaluated aPCC in 3 patients with major bleeding receiving apixaban and 8 receiving rivaroxaban.19 All patients were receiving an FXaI for atrial fibrillation, and 2 patients had a concomitant diagnosis of venous thromboembolism. Only patients presenting with an intracranial bleeding event documented via computed tomographic scans were included. The patients were treated with factor VIII inhibitor bypassing agent (20 U/kg). Progression of major bleeding was assessed via repeated computed tomography in 91% of patients between 8 and 24 hours after initial imaging. Of these, 40% had worsening intracranial hemorrhage on repeat imaging. Overall, 27% died before discharge from the hospital, and 18% developed a thrombotic complication during their admission. It was not possible to provide a rate of all-cause mortality and thrombosis, because the length of follow-up for the cohort was not provided.
Andexanet alfa
ANNEXA-4 was a multicenter, prospective, open-label, single-arm study that evaluated andexanet alfa for patients receiving apixaban, edoxaban, rivaroxaban, or enoxaparin who presented with major bleeding.20 Major bleeding was defined as potentially life-threatening bleeding associated with hemodynamic compromise, a decrease in hemoglobin of ≥2 g/dL, or bleeding in a critical area or organ. Of note, patients were excluded if they were presenting with an intracranial hemorrhage and a Glasgow Coma Scale score <7, a hematoma volume estimated to be >60 mL, an expected survival <1 month, or thrombosis within the previous 2 weeks. The study had 2 coprimary endpoints: the percentage change from baseline in anti–factor Xa activity and the percentage of patients deemed to have good or excellent hemostasis 12 hours after andexanet infusion. The study outcomes were adjudicated independently by a committee. The safety analysis was comprised of all patients who received a dose of andexanet, including 194 patients receiving apixaban, 128 receiving rivaroxaban, and 10 receiving edoxaban. A small percentage (6%) of patients were receiving enoxaparin. Most patients were prescribed an anticoagulant for atrial fibrillation (80%). Patients presented with intracranial hemorrhage (65%), gastrointestinal bleeding (26%), or other (10%). During the 30-day follow-up, the overall mortality rate was 0.5 per 100 person-days, and the cumulative overall mortality was 14%. The 30-day thrombotic event rate was 0.4 per 100 person-days, and the cumulative incidence of thrombotic events was 10%. Most of the thrombotic events occurred before anticoagulation was restarted. Seventy-two percent of patients were deemed by independent adjudicators to have good or excellent hemostatic efficacy 12 hours after the infusion of the study drug, using criteria adapted from the Sarode et al study.18 Notably, compared with the criteria proposed by the ISTH,17 the criteria for effective hemostasis in intracranial hemorrhage were based solely on imaging results and did not include clinical deterioration or the need for repeat hemostatic products 48 hours after initial management.
This review highlights the methodologically limited evidence regarding the thrombosis and mortality risks associated with use of PCC, aPCC, and andexanet alfa for the management of FXaI-associated MBE. All studies were observational in nature, with no control groups for comparison, and therefore are at risk of selection bias with respect to included patients. Studies with retrospective data collection are also at risk of detection bias regarding outcome ascertainment and adjudication such that the true estimates of thrombosis are uncertain. Furthermore, there is insufficient evidence regarding the use of PCC or andexanet for patients treated with edoxaban or betrixaban.
Given these limitations, the pooled data on the use of PCC for the management of FXaI-associated MBE showed that 18% of patients died and 3% experienced a thrombotic complication during hospital admission. At 30 days after FXaI-associated MBE, 26% of patients had died and 6% had experienced thrombosis. The majority of the deaths occurred early after the MBE. In the 2 prospective studies of consecutive patients with centrally adjudicated outcomes, the majority of the deaths were attributed to the index bleeding event.3,5 The 30-day pooled mortality rate and cumulative incidence calculated for PCC were higher than those for andexanet, which may be due to baseline differences in patient populations. Furthermore, a substantial proportion of thrombotic events occurred after hospital discharge, suggesting that additional considerations for the development of thrombosis likely contribute to this risk, including withdrawal of anticoagulants in patients at high baseline risk for thromboembolism. In the 2 above-mentioned prospective studies, 78% of the thrombotic complications occurred before resumption of full-dose anticoagulation. These findings are consistent with those of the ANNEXA-4 study, in which half of the thrombotic events occurred beyond 5 days after the andexanet infusion, although the 30-day rate and cumulative incidence were found to be higher in the ANNEXA-4 study. This increase in thrombotic events may be related to differences in study design, particularly as they pertain to the detection of thrombotic events within a prespecified, standardized prospective follow-up period. The higher mortality rate seen in the PCC studies may also have led to a lower thrombotic event rate because patients who died would not have developed thrombosis. Of note, the cumulative incidence of thrombosis after 4F-PCC presented here is higher than that found in patients receiving warfarin, which was reported to be 1.8% in a previous meta-analysis (95% CI, 1.0–3.0).21 In 2 recent retrospective studies comparing PCC for the management of MBE in patients receiving warfarin and FXaI, however, the incidence of death and thromboembolic events did not differ significantly between the 2 groups.8,12 Therefore, the incremental contribution of PCCs and andexanet to the thrombotic risk in this setting remains uncertain.
This review has several limitations. Most of the studies were of small sample size, retrospective in nature, and at high risk of bias. Furthermore, an important selection bias was present in most of the included studies, in which the sickest patients were likely chosen to receive off-label hemostatic support agents, whereas patients with less critical bleeding or with other management options (such as local hemostatic measures) may not have been offered these interventions.
In summary, the quality of evidence for the use of PCC in FXaI-associated MBE is very low. In the event of a life-threatening bleed, it is reasonable to offer PCC for hemostatic support as an adjunct to other interventions, including FXaI cessation, promotion of adequate renal function, transfusion support, and procedural or surgical interventions to achieve local hemostasis. Evidence for aPCC is even more limited, precluding recommendations about its use in this setting. Andexanet is the only agent currently approved in the United States and Europe for management of apixaban- and rivaroxaban-associated major bleeds. However, its high cost and lack of availability remain significant challenges for its use in everyday practice. Further studies designed to randomize patients to a treatment or control group are needed to help better characterize the efficacy and safety of these interventions in the management of FXaI-MBE. The ongoing ANNEXA-I (A Phase 4 Randomized Clinical Trial of Andexanet Alfa [Andexanet Alfa for Injection] in Acute Intracranial Hemorrhage in Patients Receiving an Oral Factor Xa Inhibitor) study is evaluating andexanet compared with usual care in patients with acute intracranial hemorrhage receiving a direct oral FXaI (NCT03661528).
Recommendations
Andexanet alfa should be used for the management of apixaban- or rivaroxaban-associated intracranial or gastrointestinal major bleeding (Grading of Recommendations Assessment, Development, and Evaluation grade 2C).
4F-PCC should be administered as a hemostatic therapy for the management of apixaban-, rivaroxaban-, edoxaban-, or betrixaban-associated major bleeding (grade 2C).
There is insufficient evidence to preferentially recommend andexanet alfa or 4F-PCC on the basis of thrombosis or mortality risks (grade 2C).
There is insufficient evidence to recommend the use of aPCCs in the management of FXaI-associated major bleeding (grade 2C).
Physicians, patients, and caregivers should be advised about the uncertainty of efficacy and the risks of thrombosis and mortality associated with these 4F-PCCs and andexanet alfa for FXaI-associated major bleeding (grade 2C).
Acknowledgments
M.K. has received grant funding from the CanVECTOR network for her fellowship in adult thrombosis medicine. D.M.S. is supported by a research early career award from the Hamilton Health Sciences Foundation.
Correspondence
Deborah M Siegal, Population Health Research Institute, 20 Copeland Ave, C3-120, Hamilton, ON L8L 2X2, Canada; e-mail: siegald@mcmaster.ca.
