
Abstract
The development of BCR/ABL1 tyrosine kinase inhibitors (TKIs) over the past 20 years has dramatically improved the outcomes for patients with every stage of Philadelphia chromosome-positive (Ph+) chronic myeloid leukemia (CML). Clinicians now have access to 5 oral, generally well-tolerated, and highly effective TKIs. How should these agents be used for an individual patient to ensure the best possible duration and quality-of-life, to avoid treatment-related complications, and potentially to achieve a cure at an affordable cost? Because CML patients may need to continue TKI therapy indefinitely, the long-term safety of each treatment option must be considered. Evidence-based care requires an understanding of the optimal use of these drugs, their specific early and late toxicities, the prognostic significance of achieving treatment milestones, and the critical importance of molecular monitoring. Efficacy is important, but treatment choice does not depend only on efficacy. Choosing among various treatment options is informed by understanding the distinct benefits and risks of each agent, along with careful consideration of patient-specific factors, such as risk status, age, and comorbidities.
Learning Objectives
To compare the efficacy and safety of frontline BCR/ABL1 tyrosine kinase inhibitors in newly diagnosed chronic phase CML
To recognize the utility of risk assessment and molecular monitoring to individualize treatment
To understand the importance of early molecular response assessment with respect to long-term outcomes
A 58-year-old man presented with asymptomatic leukocytosis. His past medical history included hypertension, adequately controlled with metoprolol, and diabetes for which he took metformin. His physical exam was notable only for an enlarged spleen palpable 5 cm below the left costal margin. His white blood cell count was 128 000/μL with a predominance of neutrophilic cells, 2% blasts, 3% eosinophils, and 2% basophils. His hemoglobin was 13 g/dL and platelet count 640 000/μL. Qualitative RT-PCR for BCR/ABL1 on blood was positive for the p210 transcript. A bone marrow exam confirmed the diagnosis of chronic phase CML. His karyotype was 46 XY,t(9;22) in all 30 metaphase cells. His QT interval on electrocardiogram was within normal limits. His clinical risk score was intermediate (Sokal and Hasford) or low (EUTOS).
Is there a best TKI for this patient with newly diagnosed chronic myeloid leukemia (CML) in chronic phase? The development of tyrosine kinase inhibitors (TKIs) over the past 20 years has dramatically altered the management as well as the outcomes for patients with every stage of Philadelphia chromosome-positive (Ph+), BCR-ABL1+, CML. Over a relatively short period of time, treatment recommendations have evolved from allogeneic hematopoietic cell transplantation (alloHCT) early in the disease course or recombinant interferon-alfa (rIFNα), to the availability of 5 oral, generally well-tolerated and highly effective TKIs. Three (imatinib, dasatinib, and nilotinib) are approved for front-line use. Two others (bosutinib and ponatinib) are approved for intolerance or failure of prior TKI therapy. How should these agents be used for an individual patient to ensure the best possible duration and quality-of-life, to avoid treatment-related complications, and potentially to achieve a cure at an affordable cost? Evidence-based care requires an understanding of the optimal use of these drugs, their specific early and late toxicities, the prognostic significance of achieving treatment milestones, and the critical importance of monitoring.
Because CML patients may need to continue TKI therapy indefinitely, the long-term safety of each treatment option must be considered. Comprehensive data on both safety and efficacy are now available for imatinib after >10 years use as initial therapy and after 5-6 years for frontline use of dasatinib and nilotinib. Long-term TKI therapy can lead to the development of different types of adverse events (AEs) from those seen soon after initiating therapy. In addition, as patients age concurrent illnesses may develop or preexisting conditions may progress and become clinically important. Thus, physicians are called upon to choose among various treatment options in order to recommend the optimal therapy for each individual patient. Such decisions are informed by a detailed understanding of the distinct benefits and risks of each agent, along with careful consideration of patient-specific factors such as risk status, age, and comorbidities.
Recommendations from the European LeukemiaNet for the Management of CML4
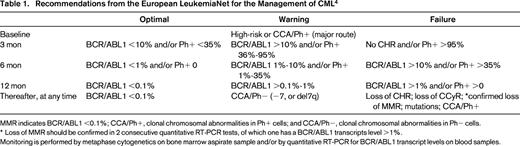
MMR indicates BCR/ABL1 <0.1%; CCA/Ph+, clonal chromosomal abnormalities in Ph+ cells; and CCA/Ph−, clonal chromosomal abnormalities in Ph− cells.
* Loss of MMR should be confirmed in 2 consecutive quantitative RT-PCR tests, of which one has a BCR/ABL1 transcripts level >1%.
Monitoring is performed by metaphase cytogenetics on bone marrow aspirate sample and/or by quantitative RT-PCR for BCR/ABL1 transcript levels on blood samples.
Randomized clinical trials
Despite the uncommon incidence of CML, a large number of multicenter, randomized clinical trials (RCTs) have been completed evaluating the frontline use of TKI therapy. These are often updated annually at international meetings and in peer-reviewed publications. The data have been analyzed in multiple comprehensive reviews and incorporated into widely-practiced guidelines.1-5 Many of these trials have been conducted by pharmaceutical company sponsors, leading to registration by health authorities; others have been designed and conducted by publically funded cooperative clinical trials groups. After imatinib was shown to be more effective and better tolerated than the previous standard therapy of rIFNα and low-dose cytarabine in the IRIS trial, imatinib has generally been the standard comparator at the initial dose of 400 mg daily for all of these trials. The experimental arms have included higher doses of imatinib, imatinib plus interferon, or one of the second generation TKIs.6-19 Whether 400 mg daily is the optimal starting dose for imatinib is not clear; some trials, but not all, have shown superior achievement of major molecular responses (MMRs) with 600 or 800 mg daily.6-11 Notably, however, there have been no randomized comparisons of the second generation TKIs against each other. Thus, we are left comparing outcomes between similar trials, anchored by one arm with imatinib 400 mg daily, in order to try to identify which second generation TKI might be better for an individual patient or a particular patient cohort. Such comparisons may be misleading.
Although RCTs are the gold standard for evidenced-based medicine, they have serious limitations. Because of stringent eligibility requirements, older patients and those with comorbid disorders have generally been excluded from these frontline studies. As a consequence, information is lacking about how best to manage patients with hepatic or renal failure, pre-existing cardiac or vascular disease, congenital QT prolongation on electrocardiogram, or gastrointestinal and malabsorption syndromes. Very large trials would be required in order to include sufficient numbers of subjects within small subsets with distinctive risk characteristics, such as older patients with cardiovascular disease plus high Sokal scores. Within prospective clinical trials, rigorous protocol-mandated follow-up emphasizes adherence, both to daily treatment and to frequent monitoring; thus, outcomes may be different when the same treatment is employed in less well-controlled daily practice. Finally, clinical trials emphasize early surrogate endpoints such as complete cytogenetic remission (CCyR), major molecular response (MMR, BCR-ABL ≤0.1%IS), and early molecular response (EMR). Additional follow-up over many years is required to know which of these responses translate into improved progression-free survival (PFS) and overall survival (OS). From a patient's perspective, the latter is arguably the most important endpoint.
Outcomes from frontline trials
In the multi-arm German CML IV study, newly diagnosed CML patients received imatinib as initial therapy at either 400 mg daily, 800 mg daily, or 400 mg plus either interferon or cytarabine.6,7 These patients have now been followed for ∼12 years. After a median follow-up of 7.1 years, 965 patients (64%) were still receiving imatinib and 329 (22%) had switched to a second generation TKI. The probability of progression to blast crisis (BC) was 5.6% (95% CI, 4.3%-7.7%) with the frequency declining after the first year. At 10 years, PFS was 82%; OS was 84%; 89% had achieved MMR and 72% MR4.5. Faster and deeper responses were achieved with imatinib 800 mg daily. Over the first 8 years, 76% of patients had reported AEs of any grade, 22% had grade 3 or 4 AEs, 73% had nonhematologic AEs, and 28% had hematologic AEs. More AEs were observed with imatinib 800 mg daily and with imatinib 400 mg plus rIFNα. Late toxicities were not observed.
Five- and 6-year outcome data have recently been published for the ENESTnd trial and the DASISION trial, the primary registration studies for the frontline approvals of nilotinib and dasatinib, respectively.13,15,16 The Evaluating Nilotinib Efficacy and Safety in Clinical Trials-Newly Diagnosed Patients study (ENESTnd) was recently amended to continue to follow subjects for 10 years. In this industry-sponsored trial, newly diagnosed chronic phase CML patients were randomized to nilotinib 300 mg twice daily (n = 282), nilotinib 400 mg twice daily (n = 281), or imatinib 400 mg once daily (n = 283). “On core treatment” analyses included all events that occurred during core treatment with the assigned study drug. “On study” analyses included all events that occurred either during core treatment, a preplanned extension treatment, or post-protocol treatment follow-up.
After a minimum of 6 years, more patients remained on core treatment in the nilotinib 300 and 400 mg arms than in the imatinib arm (53.5%, 55.2%, and 44.9%, respectively).15,16 Reasons for discontinuation were relatively balanced across the arms with a somewhat higher fraction discontinuing imatinib due to inadequate response. In both nilotinib arms, cumulative rates of MMR and MR4.5 by 6 years were higher than in the imatinib arm. In all 3 arms, MR4.5 rates by 6 years were highest in patients with BCR-ABL1 ≤1%IS at 3 months [73.6% (106/144), 75.0% (102/136), and 72.1% (31/43), respectively] and lowest in patients with BCR-ABL1 >10%IS at 3 months [8.3% (2/24), 21.4% (6/28), and 15.9% (14/88), respectively]. More patients on nilotinib compared with imatinib achieved BCR-ABL1 ≤1%IS and fewer patients on nilotinib than on imatinib had BCR-ABL1 >10%IS at 3 months.
By 6 years, fewer patients on nilotinib than imatinib had progressed to accelerated phase/blast crisis (AP/BC).15,16 Only a single patient progressed to AP/BC on study in the sixth year of follow-up (on the nilotinib 300 mg arm, about 5 years after discontinuation from core treatment). Fewer deaths due to advanced CML have occurred in the nilotinib arms than in the imatinib arm. In the sixth year of the study, no deaths due to advanced CML occurred in any arm. Notably, compared with the overall survival at 6 years of 91% on the imatinib arm, there was no significance difference in the survival on the nilotinib 300 mg BID arm (92%).
In a second randomized trial with the same design that enrolled 267 Chinese patients, the MMR rate was 52% at 12 months with nilotinib compared with 28% with imatinib.17 However, rates of both CCyR (84% vs 87%) and freedom from progression (95% each) were similar at 24 months.
In the DASISION trial, patients with newly diagnosed CML in chronic phase were randomized to receive dasatinib 100 mg once daily (n = 259) or imatinib 400 mg once daily (n = 260).13 The primary endpoint was confirmed CCyR by 12 months. As recently reported, after 5 years, 61% of dasatinib-treated patients and 63% of imatinib-treated patients were still on their initial study drug. The rate of CCyR by 5 years was similar with dasatinib and imatinib (83% vs 78%, P = 0.19), but the rates of MMR (76% vs 64%, P = 0.002) and MR4.5 (42% vs 33%, P = 0.025) were higher with dasatinib by 5 years. Times to CCyR and MMR were significantly faster with dasatinib. There were fewer cases of transformations to either AP or BC on study or after discontinuation for dasatinib (n = 12/259; 4.6%) compared with imatinib (n = 19/260; 7.3%). However, 5-year PFS and OS rates were not different between treatment arms [PFS: 85% (dasatinib), 86% (imatinib); OS: 91% (dasatinib), 90% (imatinib)]. A higher proportion of patients on dasatinib (84%) achieved an EMR (BCR-ABL1 ≤10%IS at 3 months) compared with those on imatinib (64%). Patients who achieved an EMR at 3 months had improved PFS, OS, and lower rates of transformation to AP/BC over the 5 year period than those who did not have EMR [for dasatinib: PFS: 89% vs 72%, P = 0.0014; OS: 94% vs 81%, P = 0.0028; transformation, n = 6/198 (3%) compared with n = 5/37 (14%); and for imatinib: PFS: 93% vs 72%, P < 0.0001; OS: 95% vs 81%, P = 0.0003; transformation, n = 5/154 (3%) vs n = 13/85 (15%)]. Three new mutations were observed in the fifth year among the dasatinib-treated patients (a total of 15 patients within 5 years).
Bosutinib, another oral, dual SRC and ABL1 TKI, was evaluated in the frontline BELA trial (Bosutinib Efficacy and Safety in Newly Diagnosed CML), and results after a minimum of 2 years follow-up have been published.18 Newly diagnosed patients were randomized to receive either bosutinib 500 mg/d (n = 250) or imatinib 400 mg/d (n = 252). The cumulative CCyR rates by 24 months were similar (bosutinib, 79%; imatinib, 80%); cumulative MMR rates were 59% for bosutinib and 49% for imatinib. Responses were durable; 151/197 (77%) bosutinib patients compared with 172/204 (84%) imatinib patients remained on treatment and maintained CCyR, and 125/153 (82%) bosutinib responders compared with 117/131 (89%) imatinib responders maintained MMR. No new cases of transformation to AP/BC were observed in the second year with bosutinib; four occurred with imatinib. EMR was associated with better CCyR and MMR rates by 12 and 24 months in both treatment arms.
Results from the EPIC trial were also reported this year.19 This was a multicenter, randomized trial of ponatinib (45 mg daily) compared with imatinib (400 mg daily) in newly diagnosed, chronic phase CML. The trial was terminated early because of emerging reports of arterial thrombotic events in earlier ponatinib trials, and the follow-up of study subjects ended. Consequently, none of the prospectively defined endpoints could be determined in EPIC.
At the time of study termination, 307 patients had been randomized.19 When reported, the median follow-up was only about 5 months (range, 0-17.6). Groups were well-balanced with respect to sex, age, and Sokal score; however, the proportion of patients with one or more cardiovascular risk factors (hypertension, hypercholesterolemia, diabetes, obesity, and smoking) was higher in the ponatinib arm (n = 97, 63%) compared with the imatinib arm (n = 79, 52%). Data were available on 306 treated patients (154 ponatinib, 152 imatinib). Fourteen ponatinib and 2 imatinib patients discontinued due to AEs. Molecular response rates for ponatinib were uniformly higher compared with imatinib for all response measures and at all time points. The percentage of patients who achieved an EMR was significantly higher on the ponatinib arm compared with the imatinib arm overall, and also when patients were stratified by high-risk, intermediate-risk, and low-risk Sokal score. The percentage of patients who achieved MMR, MR4, and MR4.5 at any time in all Sokal risk groups was higher for ponatinib than imatinib. Despite early termination and short follow-up, these preliminary data suggest that ponatinib has improved efficacy over imatinib in newly diagnosed CML patients, but this drug has a higher AE rate, including arterial thrombotic events at the dose studied. Future investigations of ponatinib are planned using lower doses and additional analyses of relevant risk factors.
Early molecular responses (EMRs)
With each of the TKIs, a rapid response has been shown to correlate with longer-term clinical outcomes, both in frontline use and also after imatinib failures.4,7,20-25 There has been increasing interest in validating early molecular assessments as predictors of long-term outcomes.26 Data from multiple frontline trials indicate that a rapid decline of the BCR/ABL1 transcript level in peripheral blood cells at 3 (<10%IS) or 6 months (<1%IS) is correlated with higher rates of subsequent MMR and with better overall survival.4,26 Other measurements, such as a half-log reduction of baseline BCR-ABL1 transcript levels or a halving time ≤76 days, emphasize the dynamic nature of this process.26,27 These calculations, which require a control gene other than ABL1 in the PCR lab, have been recently reviewed by Deininger.28 However, it is not yet clear whether altering therapy based on the lack of an EMR leads to better outcomes, although this seems like a reasonable strategy to consider.29,30
In the TIDEL-II study, newly diagnosed patients began therapy with imatinib 600 mg per day.30 Treatment for those failing to achieve prespecified molecular targets at 3, 6, or 12 months was either escalated to imatinib 800 mg/d or switched to nilotinib 400 mg BID. Only 12% of patients had >10%IS BCR/ABL1 at 3 months. After 2 years, 55% of patients remained on imatinib and 30% were taking nilotinib. At 3 years, OS was 96% and transformation-free survival was 95%. This strategy using early switching may be preferable to starting all patients on more potent TKIs considering efficacy, toxicities, and costs.
Progression events
Although there was initial concern that responses to TKIs would be quickly followed by the emergence of drug resistance in CML and subsequent progression to AP/BC, in fact, progression events have been relatively uncommon among subjects who were closely monitored on prospective studies. For most patients, molecular responses become deeper as treatment continues. This may be due in part to repeated emphasis from treating physicians and nurses that patients maintain adherence to daily dosing. Missing as few as 10% of one's imatinib doses has led to markedly reduced rates of MMR.4 Similar data are not available for second generation TKIs.
Most progression events have occurred during the first 2-3 years after initiating TKI therapy. In the ENESTnd trial, the incidence of such events within 6 years was 0.7% for those who remained on nilotinib 300 mg BID (2/282) compared with 4.2% for those who were taking imatinib (12/283; P = 0.006).31 Including those patients who had discontinued their initial protocol therapy but remained in follow-up on study, progression occurred in 3.9% of those who had been randomized to the nilotinib 300 mg BID arm (11/282) compared with 7.4% of those on the imatinib arm (21/283; p = 0.07). The incidence of progression was lowest on the nilotinib 400 mg BID arm (2.1%; 6/281; P = 0.003) compared to imatinib. During follow-up on the DASISION trial, progression to AP or BC was reported in 4.6% of patients on the dasatinib arm and 7.3% of those on the imatinib arm.13 Patients on both arms who failed to achieve an EMR by 3 months were 6-fold more likely to have a progression event.32
Overall, mutations acquired in the ABL1 kinase binding domain account for less than half of cases with loss of response to TKI therapy; progression may occur in the absence of detectable new mutations. Patients presenting in chronic phase rarely, if ever, have detectable baseline mutations.30 Nilotinib was more effective in reducing the development of mutations compared to imatinib in frontline use.31 After a minimum follow-up of 3 years on the ENESTnd trial, twice as many patients had mutations detected while on imatinib (21; 8.9%) than on nilotinib 300 mg BID (11; 4.8%) or 400 mg BID (11; 5.1%); the majority of these mutations occurred in patients with intermediate or high Sokal scores. Most mutations (14; 67%) emerging on imatinib were known to be imatinib-resistant, but still nilotinib-sensitive. The T315I mutation was rarely observed on either nilotinib or imatinib frontline treatment and 7 of 8 occurred in patients with high Sokal risk. After 2 years follow-up on the DASISION trial, 10 patients on each arm were identified to have acquired mutations. In 7 patients on the dasatinib arm, a T315I mutation was found; none of the imatinib treated patients had acquired this mutation.32
Treatment-free remissions
Patients who achieve deep and sustained molecular remissions are candidates for one of several ongoing prospective discontinuation trials. Several studies have reported that some of these patients will maintain their remission for a long period, and perhaps indefinitely, after discontinuing their TKI. It is not yet known how large this fraction may be, but it is unlikely to be the majority of newly diagnosed chronic phase patients. Initiating treatment with a more potent TKI may increase the likelihood of being able to successfully discontinue therapy subsequently. This topic was recently reviewed in detail by Deininger28 and by Mahon.33
Side effects
Side effects from TKI therapy are rarely severe, and perhaps for that reason, they tend to be minimized by clinicians. However, low grade toxicities from a therapy that patients may need to continue indefinitely can impact adherence and thus overall outcomes.32 Compared to patient-reported outcomes, physicians tend to underestimate symptom severity and overestimate the overall health status of CML patients. In a large Italian study, symptom severity was most often underestimated for fatigue (51%), muscle cramps (49%), and musculoskeletal pain (42%).34
Initial treatment with any of these potent BCR/ABL1 kinase inhibitors frequently leads to pancytopenia because, at diagnosis, blood cells from all 3 lineages are predominantly derived from the Ph+ stem cell. After the disease recedes and normal hematopoiesis recovers, these TKIs rarely cause clinically significant myelosuppression. Whether TKI therapy should be transiently suspended during early pancytopenia is uncertain, and some experts prefer to continue the TKI therapy uninterrupted and to support patients with transfusions and filgrastim until normal blood counts recover. The spectrum of early drug-related adverse effects varies between the available TKIs.3 Pre-existing comorbidities such as gastritis, gastrointestinal syndromes, hyperglycemia, fluid retention, or liver dysfunction may be made worse by some agents but less so by others. Physician judgement and ancillary supportive care are required to meet the needs of individual patients.
The failure of the more potent and efficacious second generation TKI's to significantly prolong survival over that achieved with imatinib suggests that non-CML related causes of death have become more prevalent as CML has become a manageable chronic health problem. The impact of comorbidities was studied during imatinib treatment in the German CML IV study which enrolled patients between 16 and 88 years old (median, 53 years).6,7,35 In a recent report, 1519 of these patients were analyzed by cohorts according to their Charlson Comorbidity Index (CCI) at diagnosis.35 Higher CCI was significantly associated with lower OS. At 8 years, the probabilities for OS for CCI 2, 3-4, 5-6, and >7 were approximately 94%, 89%, 78%, and 46%. Significant differences were observed even when age was excluded from the index score. In the highest comorbidity cohort, 9 patients died after progression to AP or BC, but 33 patients died without progression. No differences in remission rates or cumulative incidence of progression to AP/BC were observed between the different CCI groups, nor were there any differences in the cumulative incidences of AEs. Thus, hematologists will need to attend to patients' other health problems, as well as CML-specific therapy to improve overall outcomes. It may be possible to minimize toxicities by reducing the TKI dose in patients who have had deep molecular responses but this strategy remains to be validated.
Vascular toxicity
With longer follow-up, concern has been raised about vascular toxicities related to TKI use.37 In the ENESTnd trial, more patients in the nilotinib arms than in the imatinib arm have had vascular events, occurring at a consistent annual frequency within each arm throughout the study.16,38 At the most recent reporting, 10% of those on the nilotinib 300 mg BID arm (n = 28), 16% on the nilotinib 400 mg BID arm (n = 44), and 2.5% on the imatinib arm (n = 7) had reported ischemic heart disease, an ischemic cerebrovascular event, peripheral arterial disease, or another vascular toxicity.16 On the other hand, pleural effusions, pericardial effusion, or pulmonary edema was uncommon. In contrast, the total incidence of pleural effusion on the DASISION trial continued to increase each year in dasatinib-treated patients (29% overall).13 Most cases of pleural effusion were grade 1 or 2 (n = 67 and 74), and the median time to first grade 1 or 2 pleural effusion was 114 weeks (range, 4-299 weeks). Discontinuation of dasatinib due to pleural effusion occurred in only 15 patients (6% overall). Reducing the dasatinib dose to 50 mg per day in responding patients may reduce the incidence of pleural effusions. Arterial ischemic events were not common on this study, occurring in 12 patients (5%) on dasatinib and 6 patients (2%) on imatinib. Fourteen dasatinib-treated patients experienced pulmonary hypertension by 2D echocardiogram, but right heart catheterization was performed in only one. Cardiovascular adverse events were similar in both arms of the BELA study (bosutinib vs imatinib).18 In the EPIC trial that was terminated early, 11 (7%) ponatinib and 3 (2%) imatinib patients experienced arterial thrombotic events, designated as serious for 10 (7%) ponatinib and 1 (0.7%) imatinib patient(s).19 One patient on the ponatinib arm experienced a serious venous thromboembolic event; there were none on the imatinib arm. Ten of 11 ponatinib patients, and 2 of 3 imatinib patients with arterial thrombotic events had 1 or more cardiovascular risk factors.
Financial toxicity
An ever-expanding cohort of CML patients is currently recommended to take daily TKI drugs life-long. The financial impact of this extremely expensive therapy for individual patients as well as for entire healthcare systems has been raised by hematologists who treat this disease.39 It has been reported that patients with higher copayments for medications are more likely to discontinue or be nonadherent to TKI therapy.40 The potential impact on health system spending levels for CML after generic imatinib becomes available (in early 2016 in the United States) is the subject of considerable interest.41 The extent of the potential savings largely depends on whether and to what extent prices decline and the use of imatinib stays the same or even increases. Economic cost-effectiveness models strongly favor starting all newly diagnosed chronic phase CML patients on less expensive generic imatinib once it becomes available, and then switching to a more potent second-generation TKI for failure to achieve clinically important milestones or for intolerance.42
Evolving treatment strategies for the future
In the near future, the choice of initial TKI is likely to be driven by two facts; one clinical (because survivals appear equivalent despite differences in efficacy), and the other financial (the price of generic imatinib is likely to fall to 20%-30% of the cost of the branded drug and the second generation TKIs). Equally important determinants for which drug to use for an individual patient include tolerance (because it influences treatment adherence as well as quality-of-life), comorbidities and thus potential late complications, calculated risk status at diagnosis, and the achievement of EMR. Eventually, gene expression profiling may give us a better way to identify which patients require a second generation TKI from the outset. For now, appropriate monitoring and the use of guidelines regarding when to switch is the key to optimizing outcomes.
Side bar: how I treat chronic phase CML
My diagnostic evaluation begins with a medical history, concentrating on performance status, current and potential comorbidities, cardiovascular risk factors, and concomitant medications. I check the blood pressure and assess spleen size by palpation and measure its extension below the left costal margin. The laboratory evaluation begins with a complete blood count and WBC differential, a comprehensive metabolic panel and LDH level to check for other medical problems, and a qualitative PCR assay of the blood for BCR/ABL1. If the latter is positive, then I proceed to a bone marrow aspiration and biopsy to determine the stage of CML morphologically and obtain a sample for metaphase cytogenetics. I calculate and record the Sokal score. I obtain a baseline ECG to measure the QT interval. I do not order quantitative RT-PCR for BCR/ABL1 transcripts at diagnosis because my PCR laboratory uses ABL1 as the control gene, which affects the accuracy of any measurement >10%. I also do not order ABL1 kinase domain mutation testing at diagnosis for patients in the chronic phase because it is so rarely positive. If patients are symptomatic from leukocytosis or splenomegaly, I begin treatment with hydroxyurea and allopurinol.
I generally begin TKI therapy with imatinib at 400 mg once daily with the largest meal of the day together with an extra glass of water. This choice is based largely on the well-documented track record for this drug over the past 15 years, the lack of late complications, and the well-established methods of managing early treatment-related toxicities. The most common of these are fluid retention, gastritis, diarrhea, rash, fatigue, and myalgia. A brief drug-holiday lasting 4-5 days is often the easiest way to relieve rash, diarrhea, or myalgia; they often do not recur. In 2016, as generic imatinib becomes available in the United States, cost and formulary restrictions may become the most compelling reasons to begin TKI treatment with imatinib. During the first month on treatment, I see patients at least weekly to assess and manage adverse events and to check blood counts. Most patients will be in hematologic remission after 1-2 months. I would use transfusions or filgrastim to maintain adequate blood counts rather than interrupt imatinib for cytopenias.
For patients with a high Sokal score, I prefer to start treatment with either dasatinib or nilotinib. This recommendation depends largely on the greater potency of these agents, which has led to higher rates of EMR and MMR. The choice between these 2 second-generation TKIs is governed mostly by their side effect profiles. I would avoid dasatinib for a patient with prior lung disease or gastrointestinal bleeding. Nilotinib would not be my first choice for a patient with poorly controlled diabetes, hepatic disease, or significant cardiovascular risk factors. In the absence of comorbidities or risk factors, the choice between these 2 drugs is left to patient preference for either a once per day medication versus one that is taken twice per day on an empty stomach.
I follow the European LeukemiaNet recommendations and obtain a quantitative RT-PCR assay on the blood after 3 months. If the patient has achieved an EMR (<10%IS) and is tolerating their initial TKI, then I continue the current therapy, and repeat the monitoring every 3 months. For imatinib-treated patients who do not achieve an EMR at 3 months, I recommend switching to a second generation TKI. For patients who have not yet achieved a hematologic remission by 3 months, I would repeat a bone marrow exam with cytogenetics, looking for evidence of accelerated phase disease. I would also look for emergence of an ABL1 kinase domain mutation as this might guide the choice for the next TKI. Patients who are resistant to 2 TKIs or intolerant to 3 should be considered for an allogeneic transplant while still in chronic phase.
Correspondence
Richard A. Larson, Section of Hematology/Oncology, The University of Chicago, 5841 S. Maryland Ave, MC-2115, Chicago, IL 60637; Phone: 773-702-6783; Fax: 773-702-3001; e-mail: rlarson@medicine.bsd.uchicago.edu.
