
Abstract
Allogeneic transplantation constitutes curative treatment for acute myeloid leukemia and myelodysplastic syndrome. Its therapeutic effects are to a large extent mediated by GVL effects, but partially offset by treatment-related mortality and loss of quality of life caused by acute and chronic GVHD. Although severe acute and chronic GVHD are associated with a reduction in relapse risk, they are not associated with improved survival. Recent efforts to modulate the GVL-GVH balance include novel methods of in vitro or in vivo T-cell depletion that are associated with a minimal impact on rates of disease recurrence and a dramatically decreased risk for GVHD. Donor selection algorithms may also have a significant impact on transplantation outcomes. Low-expression HLA alleles, particularly HLA-DP, should be incorporated in selection of adult unrelated donors. Evolving data suggest that KIR typing may also be important. High-resolution HLA typing and the importance of fetal-maternal interactions in umbilical cord blood transplantation are also briefly discussed. A combination of donor selection strategies and GVHD prophylaxis methods will favorably affect long-term outcomes and create an environment suitable for effective posttransplantation interventions.
Introduction
The importance of GVL effects constitutes a central tenet of transplantation supported by the classic observations of (often transient) remission induced by donor lymphocyte infusion after relapse. Randomized studies and cohort comparisons consistently show superior survival after allogeneic transplantation compared with conventional chemotherapy for acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS) with intermediate and adverse prognostic characteristics.1-3 However, allogeneic transplantation is used for only a fraction of patients with AML in part due to the lack of matching sibling or unrelated donors and in part to the real or perceived acute and chronic toxicity of transplantation. In one survey, GVHD and its sequelae were the most important deterrent from transplantation.4 If the sequelae of GVHD could be prevented while maintaining cure rates, the acceptance and utility of allogeneic transplantation would increase. In patients with AML and MDS, can one avoid toxicity and late sequelae of transplantation without sacrificing rates of recurrence? Older observations correlate disease control with occurrence of acute GVHD (aGVHD) and chronic GVHD (cGVHD),5 but many patients in such studies received transplantations for chronic myeloid leukemia, a disease much more susceptible to GVL mechanisms. More recent observations highlight the detrimental aspects of GVHD, particularly of cGVHD. A study from Seattle of 1092 patients undergoing nonmyeloablative transplantation (median age 56, median follow-up 5 years, n = 381 with AML or MDS) found that cGVHD but not aGVHD was associated with decreased rates of disease recurrence. However, that study also found that both severe e aGVHD and cGVHD were associated with increased nonrelapse mortality. As a result, despite lower rates of disease recurrence, cGVHD was associated with worse overall survival outcomes.6 A Center for International Blood and Marrow Transplant Research (CIBMTR) study of 4022 patients with AML and MDS (median age 42, median follow-up 4 years) similarly failed to find any survival benefit for patients with GVHD. Among recipients of myeloablative transplantation, relapse rates were reduced in those with cGVHD but not aGVHD. However, overall survival was worsened by the presence of either cGVHD or aGVHD. Among recipients of reduced-intensity conditioning transplantations, relapse rates were reduced by either cGVHD or aGVHD. However, both cGVHD and aGVHD also increased nonrelapse mortality and overall survival was worse in those with either cGVHD or aGVHD.7 A European Group for Blood and Marrow Transplantation (EBMT) analysis of patients with AML undergoing nonmyeloablative transplantation (median age 56, median follow-up 28 months) came to somewhat different conclusions. They found that both cGVHD and aGVHD were associated with decreased rates of disease recurrence. Overall survival was improved only for those with grade 1 aGVHD and limited cGVHD. Those with grade 2 aGVHD or extensive cGVHD had similar survival and those with grade 3-4 aGVHD had worse survival than those without GVHD.8 The discrepancy with the Seattle and CIBMTR data might be explained by the focus on patients with limited cGVHD, but also by the shorter follow-up in the EBMT patients, because the detriment of cGVHD becomes more apparent as time goes by.6 cGVHD continues to exact a high toll even years after transplantation.9 Twenty percent of 2-year survivors with cGVHD died between 2 and 12 years after transplantation, as opposed to 5% of those without GVHD. At this late stage after transplantation, the persistent presence of cGVHD is associated with increased risks for skin cancer, osteoporosis, cardiovascular disease, and worsened quality of life. The beneficial effects of cGVHD on relapse in AML are thus modest at best and come at a steep price. Many efforts are ongoing to affect the balance between GVL and GVHD. Here we will focus on 2 important clinical strategies: (1) pretransplantation interventions to reduce GVHD by in vitro or in vivo T-cell depletion and (2) donor selection strategies that may affect the balance between GVHD and GVL.
In vitro T-cell depletion
The first attempts at decreasing cGVHD depended on the physical removal of those cells most responsible for GVHD, namely the mature T cells, before infusion of the cells. Various methods of in vitro T-cell depletion have been used (Table 1) and early results of both positive and negative selection methods were summarized by Ho and Soiffer.10 T-cell depletion was felt to cause less aGVHD, was associated with more rapid hematopoietic recovery (mainly because posttransplantation methotrexate [MTX] can be avoided when T-cell depletion is used), and fewer early complications. However, higher rates of graft failure/rejection, higher incidence of CMV, increased risk of posttransplantation lymphoproliferative disease, and a modest increase in relapse risk offset these advantages. These observations were confirmed in a large randomized study of unrelated donor transplantation conducted between 1995 and 2000, which showed equivalent results after in vitro T-cell–depleted BM transplantation followed by posttransplantation cyclosporine compared with transplantation of unselected donor grafts followed by posttransplantation cyclosporine and MTX.11 Approximately one-quarter of patients in this study had AML and their relapse rate was similar after T-cell–depleted versus unselected transplantation.
Studies comparing T-cell depletion with conventional GVHD prophylaxis
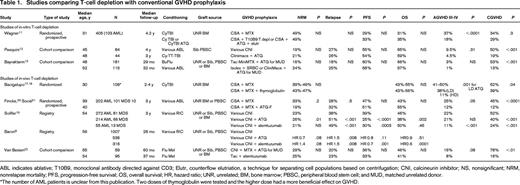
ABL indicates ablative; T10B9, monoclonal antibody directed against CD3; Elutr, counterflow elutriation, a technique for separating cell populations based on centrifugation; CNI, calcineurin inhibitor; NS, nonsignificant; NRM, nonrelapse mortality; PFS, progression-free survival; OS, overall survival; HR, hazard ratio; UNR, unrelated; BM, bone marrow; PBSC, peripheral blood stem cell; and MUD, matched unrelated donor.
*The number of AML patients is unclear from this publication. Two doses of thymoglobulin were tested and the higher dose had a more beneficial effect on GVHD.
Since the 1990s, the diagnosis, prevention, and treatment of CMV and Aspergillus have much improved and the risk of graft rejection may be mitigated by the use of G-CSF–mobilized peripheral blood stem cells. Recently, several groups have compared the outcome after T-cell–depleted allotransplantation with that after conventional GVHD prophylaxis in AML and MDS patients. Pasquini et al compared the outcomes of AML patients undergoing myeloablative conditioning and transplantation of a CD34-selected unrelated graft, (Clinimacs; Miltenyi-Biotec) with that of similar patients receiving unselected grafts.12 The Clinimacs device typically results in profound T-cell depletion and the patients receiving CD34-selected grafts did not receive calcineurin inhibitors after transplantation. The 100-day rates of grade 2-4 aGVHD were 23% with T-cell–depleted grafts and 39% with conventional immune suppression (P = .07). The 2-year rates of cGVHD were lower with T-cell–depleted grafts (19% vs 50%, respectively; P < .001). There were no differences in rates of graft rejection, leukemia relapse, treatment-related mortality, or disease-free and overall survival rates. At 1 year, 12% and 54% of patients were still on immunosuppression in the T-cell–depleted and conventional immunosuppression cohorts, respectively.
Bayraktar et al compared the outcomes of patients with AML in CR1 undergoing allotransplantation at Memorial Sloan-Kettering Cancer Center (MSKCC) using in vitro T-cell depletion without posttransplantation GVHD prophylaxis with that at MD Anderson Cancer Center (MDACC) using unmanipulated stem cells and conventional GVHD prophylaxis consisting of tacrolimus and mini MTX (5 mg on days 1, 3, 6, and 11).13 Two methods of T-cell depletion were used consecutively at MSKCC. For the first cohort of patients, initial CD34 selection with the Baxter Isolex device was followed by a second step of sheep RBC rosetting. Subsequently, 22 patients received a CD34-selected graft using the CliniMacs device. At both centers, patients with unrelated donors received horse or rabbit antithymocyte globulin (ATG). T-cell depletion graft recipients were more likely to be older, receive a mismatched transplantation, and have peripheral blood used as the graft source. The rate of grade 2-4 aGVHD occurring within 100 days after transplantation was significantly lower in the T-cell–depleted graft group (5% vs 18%, P = .005). There was no significant difference in the rate of grade 3-4 aGVHD between the 2 groups (1% vs 3%, P = .3). The rate of cGVHD was lower in the T-cell–depleted graft group (13% vs 53%, P < .001). Three-year relapse-free and overall survival rates were 58% and 57% in recipients of T-cell–depleted grafts and 60% and 66% in recipients of unmodified grafts (P = NS), respectively.
The data from these studies are consistent with those from the older studies. In vitro T-cell depletion does not significantly affect the rate of disease recurrence or survival for patients with AML or MDS in remission and results in lower rates of cGVHD and aGVHD. It can be expected that, due to the lower rate of cGVHD, quality of life will be better among survivors and that very long-term survival may be improved. In recent studies, graft failure no longer constitutes a major problem and, with modern supportive care, the rate of serious opportunistic infections does not seem to be increased.
In vivo T-cell depletion
Another approach to functionally effect T-cell depletion consists of the administration of T-cell–directed antibodies (Table 1). For this purpose, the anti-CD52 antibody alemtuzumab or 1 of 3 forms of ATG, Thymoglobulin (rabbit), Atgam (equine), or ATG Fresenius (ATG-F; rabbit directed against the Jurkat cell line), are commonly used. These products are by no means interchangeable, but unfortunately very few studies have compared their relative merits and few of them have addressed the complexities of dosing.
Equine ATG is the oldest product and remains the standard of care in treatment for severe aplastic anemia, but has largely been replaced in allogeneic transplantation in the United States by Thymoglobulin, which has higher affinity for human lymphocytes and an extended half-life. A retrospective single-center comparison showed that Thymoglobulin was a much more powerful immunosuppressant with less cGVHD or aGVHD but a higher risk for opportunistic infections.14 ATG-F and Thymoglobulin are both derived from rabbits, but ATG-F has a lower concentration of active antibodies and higher doses tend to be used. In one study, the use of either preparation was associated with decreased rates of cGVHD and similar survival compared with nondepleted transplantations, but ATG-F at the doses used seemed more efficacious.15 Another retrospective study suggested better preservation of GVL effects after ATG-F compared with Thymoglobulin.16
Several randomized studies of the use of ATG have been conducted, particularly in unrelated donor transplantation. An older study by Bacigalupo et al showed a reduced risk for grade 3-4 aGVHD and a reduced risk of cGVHD with the use of Thymoglobulin, but no effect on treatment-related mortality or long-term outcome.17 An update of this study showed impressive benefits of ATG among long-term survivors, with a lower incidence of chronic lung dysfunction, better Karnofsky Performance Status, and a much lower incidence of death occurring beyond 1 year after transplantation.18 A European consortium more recently conducted a prospective study of unrelated myeloablative donor stem cell transplantation comparing GVHD prophylaxis using pretransplantation ATG-F and posttransplantation tacrolimus with conventional GVHD prophylaxis of tacrolimus and MTX. A total of 202 patients with a median age of 40 years were randomized; 101 patients had AML, 10 had MDS, and 70 had acute lymphoblastic leukemia. Only 17 patients in this series had chronic myeloid leukemia. The cumulative incidence of extensive cGVHD after 3 years was 12.2% in the ATG-F group versus 45.0% in the control group (P < .0001). The 3-year cumulative incidence of relapse and of nonrelapse mortality was 32.6% and 19.4% in the ATG-F group and 28.2% and 33.5% in the control group (P = .47 and P = .18), respectively. Overall survival rate after 3 years was 55.2% in the ATG-F group and 43.3% in the control group (hazard ratio = 0.84, P = .39). The 3-year probability of survival free of immunosuppressants was 52.9% and 16.9% in the ATG-F versus the control groups, respectively (P = .0001). A similar study is currently ongoing in the United States.
The results of this randomized study contrast with those of a large CIBMTR analysis of reduced intensity conditioning.19 That study evaluated 1676 patients, half of whom received conventional GVHD prophylaxis and ∼37% of whom received ATG. Rates of grades 2-4 and grades 3-4 aGVHD were similar, but rates of cGVHD were lower with ATG-containing regimens (40% vs 52%, P < .001). Nonrelapse mortality (26% vs 23%, P = .01) and relapse rates (49% vs 38%, P < .001) were higher for those receiving ATG. Unfortunately, in this analysis, no attempt was made to distinguish the types of ATG administered. One-third of patients received equine ATG. Compared with rabbit ATG, the risks of grades 2-4 aGVHD (P = .03) and grades 3-4 aGVHD (P = .01) were higher with horse ATG; there was no difference in cGVHD (hazard ratio = 1.03, P = .85). Nonrelapse mortality risk was higher with equine ATG compared with rabbit ATG (P = .004). Therefore, it remains unclear whether the inferior results observed with ATG are to be attributed to equine ATG or to all ATG formulations. An EBMT analysis of reduced-intensity conditioning found that in vivo T-cell depletion with ATG was associated with a higher risk of relapse, a trend for lower nonrelapse mortality, similar leukemia-free survival, and similar overall survival.8
Alemtuzumab is a monoclonal antibody directed against CD52, an antigen expressed on all lymphocytes. Alemtuzumab has been used extensively in GVHD prophylaxis for transplantation.20 One obvious advantage over ATG preparations is the decreased risk of posttransplantation lymphoproliferative disorder associated with its use.21 No randomized studies involving alemtuzumab have been reported.
We compared outcomes of fludarabine-melphalan reduced intensity conditioning for allotransplantation in AML and MDS using pretransplantation alemtuzumab followed by posttransplantation single-agent tacrolimus at the University of Chicago with that of patients receiving a similar conditioning regimen with conventional tacrolimus and mini-MTX at MDACC. Unrelated donor recipients at MDACC also received ATG. Both groups had similar patient and donor characteristics. There were no significant differences in treatment-related mortality, relapse, survival, or disease-free survival between the 2 groups. The incidence of aGVHD grades 2-4 (P = .01) and cGVHD (P = .01) were significantly lower in patients receiving alemtuzumab. Overall survival and nonrelapse mortality were similar between the groups.22 In the previously cited CIBMTR analysis, 12% of 1676 patients received GVHD prophylaxis with alemtuzumab. Compared with T-cell–replete regimens, day 100 rates of grades 2-4 and grades 3-4 aGVHD were lower with alemtuzumab-containing regimens (40% vs 19%, P = .001, and 22% vs 11%, P = .001, respectively). The risk of developing grades 2-4 and grades 3-4 aGVHD was also lower compared with ATG-containing regimens (P = .001). Compared with T-cell–replete regimens (52%) and ATG-containing (40%) regimens, the 3-year rates of cGVHD were lower with alemtuzumab-containing regimens (24%, P = .001). Compared with T-cell–replete regimens (23%), 3-year rates of nonrelapse mortality were similar after alemtuzumab-containing regiments (21%). The use of alemtuzumab-containing regimens was associated with higher rates of recurrence (P < .001), lower disease-free survival (P = .003), but similar overall survival (P = .46) to that of patients receiving undepleted transplantations. In contrast, an EBMT analysis showed worse overall survival for patients with AML and MDS receiving alemtuzumab-based conditioning and reduced-intensity transplantation.8
Insofar as it is possible to reconcile the results from multiple studies using drugs with very different characteristics, one can conclude that, in general, in vivo T-cell depletion is safe and that it reduces aGVHD and particularly cGVHD. The impact on the rates of disease recurrence varies from study to study and is modest at worst. The data with ATG-F are compelling, but require confirmation (studies are currently ongoing). Among ATG preparations, equine ATG appears to be less suitable for use in transplantation.
Other approaches to preventing GVHD
Current treatments to prevent GVHD invariably reduce GVL effects and are profoundly immunosuppressive. Both cellular and pharmacological treatments with improved therapeutic ratios are being studied. Examples include conditioning regimens that favor expansion of natural killer T (NKT) cells,23 or the infusion of regulatory T cells in the setting of haploidentical or cord blood transplantation.24,25 Although in the early stages of development, such treatments hold great promise.
Donor selection
The risk for GVHD is affected by genetic or acquired characteristics of the donors and/or the recipient. In unrelated donor transplantation, the genetic characteristics of the donor, particularly HLA and killer inhibitory receptor (KIR) types, and maternal effects on donor immunity may be used to improve transplantation outcomes. Although the following discussion focuses on the effects of particular mismatches on GVHD and relapse, HLA mismatches may also constitute targets for graft rejection, particularly in patients with preexisting donor-specific antibodies.26 Most centers now routinely test recipients for the presence of HLA antibodies and avoid donors who are targeted by donor-specific antibodies.
HLA in adult stem cell transplantation
The discovery of the HLA system, its role in GVHD and graft rejection, and its mode of inheritance paved the way for sibling stem cell transplantation. In unrelated donor transplantation, most attention has been focused on the so-called high-expression HLA loci, which include HLA-A, HLA-B, HLA-C, and HLA-DR. Using modern, high-resolution typing methods, it has been shown that high-resolution typing at HLA-A, HLA-B, HLA-C, and HLA-DR predicts for transplantation outcome with adult unrelated donors. As a rule of thumb, each mismatch at HLA-A, HLA-B, or HLA-DR is associated with an ∼ 11% decrease in long-term survival (and a considerable increase in risk of cGVHD for survivors).27 However, only a limited percentage of patients have donors in the registry that are fully matched at all 8 loci. Many centers therefore accept mismatched donors. If mismatching is to be accepted, a single mismatch at HLA-B or HLA-C seems to be better tolerated after BM transplantation than mismatches at HLA-A or HLA-DR. After peripheral blood stem cell transplantation, HLA-C and HLA-A antigen mismatches and HLA-B antigen/allele mismatches were the most detrimental.28
The HLA complex contains several additional HLA genes that are expressed at lower density, the most important ones of which are the HLA-DQ genes (DQB1 and DQA1) the HLA-DP genes (DPB1 and DPA1), and the HLA-DRB3, HLA-DRB4, and HLA-DRB5 genes.29
HLA-DQB1 is in very close linkage disequilibrium with HLA-DRB1 and there are relatively few cases of isolated HLA-DQB1 mismatch. When present, an isolated DQB1 mismatch is not associated with increased risk. In contrast, the combination of a DQB1 mismatch together with an HLA-A, HLA-B, HLA-C, or HLA-DRB1 mismatch greatly increases transplantation risks.
The HLA-DPB1 gene has rather limited polymorphism, with 5 of the alleles accounting for more than 80% of the cases. However, because of its lack of linkage disequilibrium with the other HLA genes, random differences between donor and recipient HLA-DPB1 type occur in the majority of HLA-A, HLA-B, HLA-C, and HLA-DR matched transplantations. Recently, Fleishauer et al were able to distinguish permissive from nonpermissive mismatches based on in vitro reactivity. In a large analysis, they showed that permissive DP mismatches, occurring at random in ∼ 40% of donor-recipients pairs, have similar outcomes compared with those without DP mismatch. However, nonpermissive mismatches have detrimental impacts that are comparable to those of an HLA-A, HLA-B, HLA-C, or HLA-DR mismatch and should probably be avoided.30 The use of DP matching is therefore currently being added to the increasing list of determinants of transplantation outcome.
Lastly, DRB3, DRB4, and DRB5 are genes with limited polymorphisms the expression of which in humans is mutually exclusive. For practical purposes, they can therefore be considered as alleles of the same gene. Mismatching between donor and recipient at any of these antigens has little effect, but when combined with mismatches at other low-expressing loci (DQB1, DQA1, DPB1, DPA1), a detrimental effect on overall survival becomes detectable. Three or more mismatches at any of the 6 low-expressing antigens (DQB1, DQA1, DPB1, DPA1, DRB3/4/5) occur at random in ∼ 10% of the 7/8 transplants and are to be avoided.29
HLA matching in umbilical cord blood transplantation
Umbilical cord blood (UCB) grafts cause less GVHD than adult grafts and therefore more mismatching is permissible. Current standards for selecting UCB units do not typically include matching at HLA-C and emphasize UCB cell dose in addition to HLA type.31 However, a retrospective analysis of 803 mostly pediatric patients reported to CIBMTR showed that mismatch at HLA-C was associated with worse treatment-related mortality but not with increased rates of GVHD.32 A more recent analysis used high-resolution typing at all high-expression loci (HLA-A, HLA-B, HLA-C, HLA-DR). The investigators found that, after adjusting for cell dose, mismatches at any of these loci except HLA-B were associated with increased nonrelapse mortality and that the detrimental effect of mismatches was cumulative. An effect on overall survival became apparent when more than 4 loci were mismatched.33
KIR
NK cells are effector cells of the innate immune system that contribute to GVL effects, particularly in myeloid malignancies, and seemingly do not cause GVHD.34 Their biology and regulation is complex, so a complete description is beyond the scope of this chapter (for review, see Murphy et al34 ), but it is governed to a large degree by interaction of surface receptors with their cognate ligands on target cells. The best known of these receptors are the KIRs. The KIR receptor gene locus, like the HLA locus, is a multigene locus, but it is located on chromosome 19. Some KIRs, upon engagement of their cognate receptor, will mediate an inhibition of the NK cell, hence their name. However, others, the so-called activating KIRs, will send activating signals. Different KIR receptors have different cognate ligands, most of them HLA-class I molecules, particularly HLA-C (but also some HLA-A or HLA-B). In this respect, there are 2 types of HLA-C molecules serving as cognate ligands for different KIRs. HLA-C with arginine at position 80 have the so-called C1 epitope, those with lysine at position 80 have the C2 epitope (importantly, C1 and C2 in this context stand for groups of HLA-C antigens, not specific HLA-C antigens). Certain HLA-A and HLA-B characterized by Arginine at position 83, the so called Bw4 epitope, can also serve as ligands for other KIRs. There is considerable genetic diversity in the KIR gene locus, but this heterogeneity can be organized in 2 groups of haplotypes. Individuals with the so-called group A haplotypes have a gene locus enriched for genes that bind effectively to their ligands, and those with group B haplotypes have a locus enriched for genes with reduced or impaired capacity to bind to their ligands. A-haplotypes are associated with better resistance to infections, B-haplotypes with improved reproductive capacity. Lastly, the expression of KIR receptors in a particular individual is affected by the genetic presence and expression of its cognate ligand. For example, suppose a certain individual carries the gene for KIR2DL1, the cognate ligand of which is an HLA-C of C1 type, but his HLA genotype does not include such an HLA-C. In such an individual, KIR2DL1, although genetically present, is constitutionally silent—that is, it is “not licensed.” (Teleologically, if such were not the case, the lack of engagement of KIR2 DL1 by its cognate ligand would result in auto-aggression of the individual's cells.)
The relationship among KIR matching, expression, genotype, and transplantation outcome has been an area of intense interest with rapidly evolving data and insights. The potential complexity of interactions is bewildering and is influenced by donor and recipient HLA and KIR genetics as well as KIR expression (licensing), the underlying disease, and the transplantation methodology. The initial observations from Ruggeri et al used the missing ligand hypothesis35 and focused on T-cell–depleted haploidentical transplantations. Based on the HLA type of the recipient, they inferred that the ligand for licensed KIR receptors was absent in certain recipients. AML patients with a missing KIR ligand in the recipients had a much decreased rate of disease recurrence and improved survival. These early observations were confirmed by some but not all subsequent investigators.34 It is likely that the impact of missing KIR ligand is highest in situations where alloreactive T cells are lacking (eg, T-cell–depleted haploidentical transplantation).
In HLA-identical or nearly HLA-identical transplantations, other aspects of KIR physiology may take on a more important role. For example, in unrelated donor transplantation, the Minnesota group focused on the KIR genotype of the donor regardless of KIR type of the recipient. They found that those donors with at least one KIR-B haplotype (B/x, ∼ 75% of all donors) had superior outcomes to those who had KIR A/A haplotypes.36 In a subsequent analysis, they distinguished 2 subcomponents of the KIR-A and KIR-B haplotypes that tend to genetically segregate because of a unique recombination site situated approximately halfway in the locus.37 The presence of the centromeric B genes (cen B) in the donor was the most important predictor of outcome and was associated with a major reduction in relapse rate of AML. Presence of telomeric B genes (tel B) provided some protection of relapse as well. Increasing numbers of B-type genes in the donor provided superior cumulative protection against relapse in AML. This model is quite attractive because of its simplicity and because of the relative ease of determination of KIR haplotype by genetic analysis. It ignores any interaction between specific KIRs and their ligands or any issues of licensing of KIRs in donors. It also ignores any potential effects of KIR genotype in recipients.
Venstrom et al recently presented a different analysis focusing on the presence of the activating KIR gene KIR2DS1 in the donor and its effect on outcome of transplantation for AML.38 The presence of KIR2DS1 in the donor was associated with a much reduced rate of relapse unless the donor was himself or herself homozygous for HLA-C2 type antigens. The effect of KIR2DS1 on relapse is explained because it is a strong activating KIR receptor, so NK cells from such donors tend to be more activated. However, KIR2DS1 has as its cognate ligand the HLA-C2 class of molecules. As a result, donors who are homozygous for HLA-C2 type antigens have a KIR2 DS1 that is tolerized. This somewhat different model therefore emphasizes, in addition to donor genotype, the importance of the interaction between HLA and KIR in the donor.
In this rapidly evolving field, most conclusions are preliminary and the different models, somewhat contradictory between each other will require confirmation before being routinely clinically used. Consistently, the presence of activating KIR genes in the donor favorably affects recurrence rates in myeloid, but not lymphoid malignancies.
NIMAs/IPAs and parental influences on graft immunology
Note: This section is partially based on a previously published commentary.39
Another complexity of donor characteristics relates to the lifelong imprint from parental exposure, an issue with consequences that have been mostly explored in UCB transplantation and somewhat in transplantation from haploidentical related donors. It has long been known that exposure of a fetus to foreign antigens, be it from a fraternal twin or from the mother, can lead to lifelong tolerance.40,41 Fetal tolerance is most pronounced to maternal antigens and then specifically to the highly immunogenic noninherited maternal antigens (NIMAs).42 Van Rood et al were the first to speculate that exposure of UCB grafts to an HLA-mismatched transplantation recipient whose mismatched HLA antigens were identical to the maternal NIMA antigens of the UCB would result in superior outcomes. Two large studies of different datasets support this hypothesis.43,44 Transplantation of an UCB graft into a mismatched recipient expressing NIMAs results in superior outcomes compared with transplantation into a recipient who does not express NIMAs.
Another important aspect of the fetal immune system is the presence of maternal microchimeric cells.45 These maternal cells are sensitized to the fetal antigens of paternal origin, the so-called inherited paternal antigens (IPAs). Van Rood et al again speculated that exposure to those IPAs in a transplantation recipient would allow the microchimeric maternal cells to target recipient cells. They provided powerful indirect evidence that this is indeed the case.46 Recipients whose HLA type includes the UCB donor's IPA have a lower rate of disease recurrence than those whose HLA type does not include those IPAs. This hypothesis would be further supported by a direct demonstration of maternal cells in UCB.47,48
The principle of maternal sensitization and resultant GVL effects also applies in related haploidentical transplantations, in which the use of maternal donors results in much superior outcomes to that of paternal donors.49
Conclusion
Severe cGVHD and aGVHD are major causes of late posttransplantation toxicity and mortality. Stringent GVHD prophylaxis using in vitro or in vivo T-cell depletion partially addresses this issue, with only a modest impact on the rates of AML recurrence and improved long-term quality of life. The donor selection strategies and interventions described here may improve the overall risk-benefit ratio of transplantation by decreasing cGVHD and aGVHD without affecting the rates of disease recurrence or reducing them. However, disease recurrence is likely to remain a significant problem. This could be addressed in a variety of ways, including posttransplantation immunotherapy or pharmacotherapy. The feasibility of such interventions/studies is dramatically enhanced by minimizing posttransplantation GVHD.
Acknowledgment
The author thanks Dr Marcelo Fernandez-Viña for advice and helpful comments in the preparation of this manuscript.
Disclosures
Conflict-of-interest disclosure: The author declares no competing financial interests. Off-label drug use: None disclosed.
Correspondence
Koen van Besien, Weil Cornell Medical College, 525 East 68th Street, Payson Pavilion 3, New York, NY 10065; Phone: 212-746-2048; Fax: 212-746-6678; e-mail: kov9001@med.cornell.edu.
