
Abstract
Routine screening for monoclonal gammopathy of undetermined significance (MGUS) is not indicated. Despite this fact, MGUS is a common finding in medical practice. Almost all individuals diagnosed with MGUS represent incidental cases diagnosed when physicians order serum protein electrophoresis, immunofixation, or both, as part of the work-up of a number of common symptoms and laboratory abnormalities. In the absence of reliable molecular predictors of outcome, the detection of an early precursor state typically imposes a complex situation for the patient and the responsible physician—usually, it leads to a lot of questions that lack clear answers. In the past years, several novel insights have been gained in the area of multiple myeloma (MM) precursor disease. This review focuses on results from recent investigations and discusses implications for diagnostic work-up, clinical management, and patient counseling. More specifically, it sheds light on the following commonly asked questions by patients and physicians: i) what is the risk of progression from precursor to full-blown MM, and are there ways to risk-stratify patients?; ii) is MM always preceded by a precursor state, and is there anything that could or should be done to delay or prevent progression?; and iii) why do some individuals develop MM precursor diseases, and is there a reason to screen the family?
Definitions and Epidemiology
From ‘Benign Monoclonal Protein’ to Monoclonal Gammopathy of Undetermined Significance
The concept of monoclonal versus polyclonal gammopathies was initially raised in 1960 by Jan Waldenström,1 who described patients with a narrow band of hypergammaglobulinemia on electrophoresis as having a monoclonal—or M—protein. Many of these patients had multiple myeloma (MM) or macroglobulinemia, while others had no evidence of malignancy. Waldenström considered these patients to have “essential hypergammaglobulinemia” or a “benign monoclonal protein.”
Based on the observation that otherwise healthy individuals with these protein abnormalities turned out to have an excess risk of developing MM, Waldenström's macroglobulinemia, light-chain amyloidosis, or related disorders, Robert Kyle coined the term “monoclonal gammopathy of undetermined significance” (MGUS) in 1978.2 According to diagnostic criteria provided by the International Myeloma Working Group (IMWG) in 2010,3 MGUS is defined as follows (and all three criteria must be met): i) serum monoclonal protein under 3 g/dL; ii) clonal bone marrow plasma cells under 10%; and iii) absence of end-organ damage such as hypercalcemia, renal insufficiency, anemia, and bone lesions that can be attributed to the plasma-cell-proliferative disorder.
Screening studies have found MGUS to be present in approximately 3.2% of Caucasians above the age of 50 years.4 Prevalence appears to be roughly twice as high among African men, African-American women, and obese individuals.5,6 Chronic antigen stimulation7–11 and pesticide exposure have also been associated with an excess risk of MGUS/MM.12,13 Recently, a large population-based study found a 2-fold increased relative risk for MM among 37,838 first-degree relatives of 13,896 MM patients (compared with 151,068 first-degree relatives of 54,365 matched controls).14 Similarly, a 3-fold-increased relative risk for both MGUS and MM was found among 14,621 first-degree relatives of 4458 MGUS patients (compared with 58,387 first-degree relatives of 17,505 matched controls).15 These observations support a role for both susceptibility genes and immune-related factors in the causation of MGUS and MM.6–17
Although MGUS is commonly referred to as single entity in the literature, lymphoid (or lymphoplasmacytoid) MGUS and plasma-cell MGUS have distinct differences both in the clinic and in the laboratory. About 15% to 20% of MGUS tumors secrete IgM, and mostly they have a lymphoid or lymphoplasmacytoid phenotype; non-IgM (IgG>IgA>light chain Ig only>IgD>IgE) MGUS tumors have a plasma-cell phenotype.18 Primary amyloidosis belongs to the plasma-cell MGUS category, although it is characterized by pathological deposits in various tissues of monoclonal Ig light-chain fragments produced by MGUS tumors, which often include only a small number of premalignant tumor cells.18
Typically, plasma-cell MGUS tumors can progress to MM or related plasma-cell disorders, whereas lymphoid MGUS tumors progress to Waldenström's macroglobulinemia, lymphoma, or other malignant lymphoproliferative disorders.19,20 Furthermore, there is virtually no overlap of the molecular genetic events responsible for the molecular pathogenesis of the two kinds of MGUS, suggesting that lymphoid and plasma-cell MGUS are distinct biological entities.21
From ‘Multiple Myeloma Without a Progressive Course’ to Smoldering Multiple Myeloma
In 1980, Kyle was the first to describe smoldering MM (SMM) as a distinct entity—an “illness that met the criteria of MM but has not had a progressive course,” a corollary to smoldering leukemia.22 Based on six patients, he found all cases to have ≥10% bone marrow plasma cells and ≥3 g/dL of M protein without progression to MM for at least 5 years.22 Since this initial description, the diagnostic criteria for SMM have evolved. In fact, several studies of SMM have been completed using criteria ranging from including patients with mild anemia, requiring M protein less than 4.5 g/dL, marrow plasma cells above 15%, ignoring percent marrow plasma cells entirely, and requiring Bence-Jones proteinuria.23–25 Furthermore, many studies have included separate definitions of SMM and indolent MM (IMM), with IMM being described as either a “mildly symptomatic” form of MM or a form of MM in which minimal end-organ damage was clinically evident even though the patient did not report any symptoms. For example, in some studies, patients with lytic bone lesions noted on imaging who had not yet suffered a pathologic fracture were classified as having IMM.23,26 Commonly, SMM and IMM patients have been combined into the entity of asymptomatic MM, while in some studies SMM and asymptomatic MM were considered equivalent.23,24,27 Due to these varying definitions, one has to be cautious when assessing results across different studies. In fact, it is very problematic to compare SMM data collected prior to 2003, the year that the International Myeloma Working Group (IMWG) released a consensus on the specific diagnostic criteria for the known monoclonal gammopathies.28
According to the 2010 IMWG diagnostic criteria, SMM is defined as follows (and both criteria must be met): i) serum monoclonal protein (IgG or IgA) ≥3g/dL and/or clonal bone marrow plasma cells ≥10%, and ii) absence of end-organ damage such as lytic bone lesions, anemia, hypercalcemia, or renal failure that can be attributed to a plasma-cell-proliferative disorder. The IMWG guidelines do not include a definition of IMM, and the term has fallen out of use; instead, such patients meet IMWG criteria for MM.28 In the current literature, asymptomatic MM is now synonymous with SMM.28
Interestingly, excess bone resorption measured by quantitative bone biopsy and biomarkers of bone turnover suggest that bone disease not detectable by skeletal survey is present even in some MGUS patients.29,30 This finding may explain the previously reported excess risk of bone fractures in MGUS patients independent of malignant transformation.31–33 Along the same lines, smaller studies have used magnetic resonance imaging (MRI) in patients otherwise defined as having SMM, and found occult bone lesions in some patients.34 Based on a hospital-based series of 72 SMM patients showing that those with an abnormal MRI of the spine had a shorter time to MM progression, the 2010 IMWG guidelines state the following: “an MRI of the spine and pelvis is recommended because it can detect occult lesions and, if present, predict for a more rapid progression to symptomatic myeloma.”28
It is important to keep in mind that clinical criteria for end-organ damage are highly dependent on the sensitivity and specificity of the methods used to detect the damage. Most likely, the definition of end-organ damage will change in the coming years as imaging technology and molecular markers improve, and this will have a direct impact on the clinical management of patients diagnosed with MM precursor disease in the future.
The Clinical Dilemma
Risk of Progression to Multiple Myeloma
Although for the individual patient it is currently not possible to predict whether the underlying MGUS will remain benign or transform to MM, from a population standpoint the significance of MGUS has been well characterized. Based on data from the Mayo Clinic, long-term follow-up of MGUS patients reveals an average 1% annual risk of developing a lymphoproliferative malignancy.19,20 Given these facts, once diagnosed, patients must be appropriately counseled that MGUS is a premalignant entity with a relatively low risk of progression to MM or related malignancies. In addition to malignant transformation, MGUS patients also have a higher risk of several pathologic conditions, including fractures31–33 and deep vein thrombosis.35,36 In fact, these recent findings suggest that osteoclastic activation and hypercoagulation occur early in the pathogenesis of plasma-cell neoplasia rather than abruptly in early MM,31–33,35,36 supporting the development of future clinical studies aimed at developing prophylaxis for fractures and thrombosis among MGUS patients at high risk. Furthermore, recent data suggest that MGUS patients (compared with the general population) have a significantly reduced life expectancy and an excess risk of dying from bacterial infections and heart, liver, and renal diseases,37 although this may be related to the various underlying medical conditions that led to the detection of the MGUS in the first place.
In the first and largest systematic study focusing on SMM, retrospective data from 276 patients seen at the Mayo Clinic between 1970 and 1995 were collected. In that study, SMM patients had a 10% average annual risk of progression to MM for the first 5 years following diagnosis, decreasing to 3% annually for the following 5 years, and then lowering to the same 1% annual rate of progression as MGUS thereafter.38
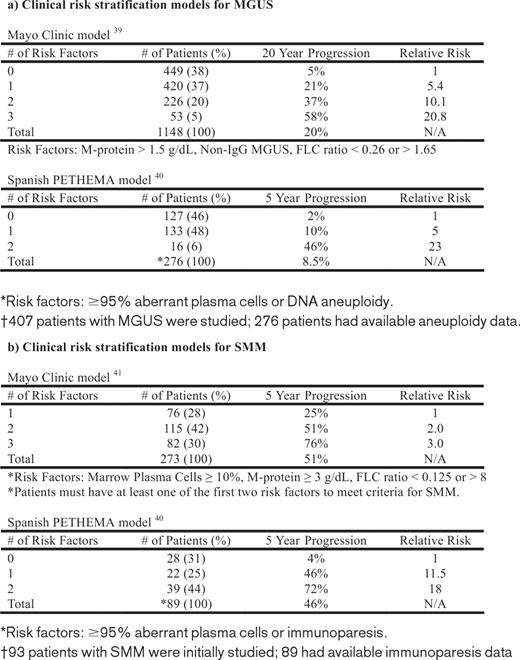
As already mentioned, we lack reliable, biological predictors of progression from MGUS/SMM to MM. In the absence of such markers, MGUS and SMM patients are currently being risk-stratified based on a few selected clinical variables that have been identified in epidemiological studies. To date, two major models have been proposed: the Mayo Clinic38,39 and the Spanish PETHEMA (Programa para el Estudio de la Terapéutica en Hemopatía Maligna)40 risk-stratification models (Table 1).
Mayo Clinic Clinical Risk-Stratification Model
The Mayo Clinic model focuses largely on serum protein abnormalities. For MGUS patients, the following features are considered to be adverse risk factors: non-IgG isotype, M-protein concentration over 1.5 g/dL, and an abnormal serum free light chain (FLC) ratio (normal reference 0.26–1.65).39 In this model, at 20 years of follow-up, MGUS patients with all three risk factors have, on average, an absolute risk of MM progression of 58%; for MGUS patients with two, one, and none of these risk factors, the corresponding absolute risk is 37%, 21%, and 5%, respectively.39 For SMM patients, the following features are considered to be adverse risk factors: ≥3 g/dL M-protein, an FLC ratio outside the reference range of 0.125 to 8, and ≥10% bone marrow plasma cells.38,41 At 5 years of follow-up, SMM patients with all three risk factors have, on average, a cumulative risk of MM progression of 76% (median time-to-progression [TTP] was 1.9 years); for patients with two or one risk factors, the corresponding risk was 51% (median TTP, 5.1 years) and 25% (median TTP, 10 years), respectively.38,41
Spanish PETHEMA Clinical Risk-Stratification Model
The Spanish model uses multiparametric flow cytometry of bone marrow aspirates to differentiate aberrant from normal plasma cells.40 Plasma cells characteristically express CD138 and intense (bright) CD38. The features of aberrant plasma cells include decreased CD38 expression, expression of CD56, and the absence of CD19 and/or CD45. In 93 SMM and 407 MGUS patients, the percentage of phenotypically aberrant plasma cells and total bone marrow plasma cells at diagnosis allowed risk stratification of MGUS and SMM patient's progression to overt MM. In their study, MGUS and SMM patients with ≥ 95% aberrant plasma cells/bone marrow plasma cells at diagnosis had a significantly higher risk of MM progression.40 Furthermore, on multivariate analysis, ≥95% aberrant plasma cells/bone marrow plasma cells, DNA aneuploidy, and immunoparesis were found to be independent predictors of MM progression. More specifically, for MGUS patients with no, one, or two risk factors (≥95% aberrant plasma cells/bone marrow plasma cells and DNA aneuploidy), the risk of progression at 5 years was 2%, 10%, and 46%, respectively. For SMM patients (risk factors: ≥95% aberrant plasma cells/bone marrow plasma cells and immunoparesis) the corresponding risks at 5 years were 4%, 46%, and 72%, respectively.40
Current Clinical Recommendations
Overall it seems reasonable to argue that MGUS cases with higher risk may benefit from annual follow-up of the M protein in addition to their usual medical care. Although the value of this has not been proven, the test is simple and worth doing, considering that MM can present with devastating bone complications that may be preventable in some patients if a significant rise in the M protein is detected in time. For SMM patients, the annual risk of MM progression is high and close monitoring has been the standard for several years.
Clearly, we need better markers to define high-risk (versus low-risk) MGUS/SMM and to better predict individual risk of MM progression. Until such markers are available, the 2010 IMWG guidelines suggest up-front risk stratification and more individualized clinical follow-up based on the above-mentioned Mayo Clinic risk-stratification model.28
In brief, the 2010 IMWG guidelines state that “low-risk MGUS” patients (M protein under 1.5 g/dL, IgG isotype, and a normal FLC ratio) should be followed with serum protein electrophoresis in 6 months, and if stable can be followed every 2 to 3 years or if symptoms arise.28 For “intermediate-/high-risk MGUS” patients (M protein above 1.5 g/dL, IgA or IgM isotype, or an abnormal FLC ratio), the guidelines state that a bone marrow aspirate and biopsy should be done at baseline to rule out underlying plasma cell malignancy; the patient should be followed with serum protein electrophoresis and a complete blood count in 6 months and then annually for life.28
For SMM patients, the IMWG guidelines state that a skeletal survey and a bone marrow aspirate and biopsy should be carried out at baseline.28 Laboratory tests and clinical work-up should be done at diagnosis and in 2 to 3 months after the initial recognition of SMM. If the results are stable, the studies should be repeated every 4 to 6 months for 1 year and, if stable, evaluation intervals can be lengthened to every 6 to 12 months; a skeletal survey should be performed if there is evidence of progression.28 Treatment is not indicated unless it is part of a clinical trial.42 For full details regarding the 2010 IMWG guidelines, please see the reference.28
Using standard chemotherapy in SMM, early treatment has not been found to delay progression to active disease and overall survival.43 The first randomized phase III study using novel drugs (lenalidomide/dexamethasone vs. surveillance) in SMM was presented by the Spanish study group at ASH 2009.44 After a median of about 1.5 years of follow-up, their interim analysis showed the following: in the surveillance arm, the progression rate was similar to historical controls, while in the treatment arm, only two patients had progressed to MM (p < 0.0001). Importantly, due to the short follow-up, the interim analysis was unable to determine if early treatment improves overall survival. Until we know the answer to this important question, we can only speculate whether early treatment has the potential to cure SMM, or if SMM should be classified as a chronic, asymptomatic disease state requiring maintenance therapy (Figure 1). At the same time, we do not know if early treatment may facilitate selection of aggressive clones that are more capable of competing in the treatment-altered microenvironment (Figure 1). Because none of these scenarios has been proven true, it is very important to conduct well-designed correlative studies in clinical trials aimed at treating SMM patients.43

Theoretically possible scenarios resulting from early treatment of smoldering myeloma. Progression of untreated high-risk SMM to full-blown MM is shown on the left. SMM patients with two or three risk factors (see Table 1) have a median TTP of 5 and 2 years, respectively. Scenarios 1 to 3 illustrate possible scenarios resulting from early treatment of SMM: Scenario 1 (center left) represents a complete cure of MM, which has not yet been reliably achieved by any current treatment modalities. This would likely require more intense treatment, necessitating improved risk-stratification of patients. Ultimately, targeted therapies may be able to achieve cure. Scenario 2 (center right) represents the generation of a chronic, asymptomatic disease state requiring ongoing maintenance therapy. This is a likely outcome of using immunomodulatory and targeted agents available in the near future. Scenario 3 (right) illustrates the theoretical possibility of the selection of a particularly aggressive, resistant clone. While TTP is extended in this scenario, overall survival may not be improved, because symptomatic disease might progress unchecked if available treatments become less effective following early treatment. Future studies are needed to fully explore these possibilities. Taken together, we do not know which, if any, of these scenarios are true. Therefore, clinical trials aimed at developing treatments for SMM should incorporate well-designed correlative studies to examine the biology of treatment response. (Reprinted with permission from Waxman et al., 2010.43 )
Theoretically possible scenarios resulting from early treatment of smoldering myeloma. Progression of untreated high-risk SMM to full-blown MM is shown on the left. SMM patients with two or three risk factors (see Table 1) have a median TTP of 5 and 2 years, respectively. Scenarios 1 to 3 illustrate possible scenarios resulting from early treatment of SMM: Scenario 1 (center left) represents a complete cure of MM, which has not yet been reliably achieved by any current treatment modalities. This would likely require more intense treatment, necessitating improved risk-stratification of patients. Ultimately, targeted therapies may be able to achieve cure. Scenario 2 (center right) represents the generation of a chronic, asymptomatic disease state requiring ongoing maintenance therapy. This is a likely outcome of using immunomodulatory and targeted agents available in the near future. Scenario 3 (right) illustrates the theoretical possibility of the selection of a particularly aggressive, resistant clone. While TTP is extended in this scenario, overall survival may not be improved, because symptomatic disease might progress unchecked if available treatments become less effective following early treatment. Future studies are needed to fully explore these possibilities. Taken together, we do not know which, if any, of these scenarios are true. Therefore, clinical trials aimed at developing treatments for SMM should incorporate well-designed correlative studies to examine the biology of treatment response. (Reprinted with permission from Waxman et al., 2010.43 )
On the Pathway from Precursor to Full-Blown Malignancy
MM is consistently preceded by a precursor state (MGUS). Although it has been known for some time now that MGUS patients have an increased risk of progression to MM and other related malignancies,19,20 it has only been recently that two independent studies have provided convincing evidence to show that virtually all cases of MM are preceded by a precursor state (MGUS).
A recent study based on 77,469 healthy adults enrolled in a U.S. nationwide population-based prospective cancer screening trial identified 71 individuals who developed MM during the course of the study. Median age at MM diagnosis was 70 years; 4.3% were African-Americans. Using serially collected, prediagnostic serum samples obtained up to almost 10 years prior to MM diagnosis, all MM cases were found to be preceded by MGUS.45 In accord with recent observations,46 the median M-protein concentration for the group exhibited a year-by-year increase over time. Two years prior to MM diagnosis, the proportion of MGUS cases with an abnormal FLC ratio was 85%, supporting a role for FLC assays in routine MGUS follow-up. Importantly, when we assessed protein abnormalities in individual patients, the following patterns were observed: in about half the study population, the M-protein concentration and involved FLC ratios showed a year-by-year increase prior to MM diagnosis, while the other half maintained largely stable abnormal serum protein level up to the diagnosis of MM (Figure 2).45 Thus, stable M-protein or FLC levels do not exclude the development of MM. Until better molecular markers for progression to MM are available, clinicians must synthesize clinical measures with routine blood tests (including renal function, hemoglobin, and serum calcium) and serum and urine M-protein markers to monitor MGUS cases.47 Although it remains to be confirmed, it has been speculated that “evolving MGUS” could potentially be an independent marker for an early myeloma with a slow rate of progression.45

M-protein concentrations year-by-year over time prior to multiple myeloma. Two major patterns of MGUS prior to multiple myeloma: “evolving MGUS” and “non-evolving MGUS.” In about half the study population, the M-protein concentration and involved FLC-ratio levels showed a year-by-year increase prior to MM diagnosis, while the other half maintained largely stable abnormal serum protein levels up to the diagnosis of MM.45 Currently, we do not know if this represents a genetic switch in the tumor cells, a change in the host, or a combination; neither do we know if these different M-protein concentration patterns represent different biology when MM arises. One might speculate that there could be differences in response to therapy and survival. Future studies need to address these and other related questions. On a clinical note, one has to keep in mind that stable M-protein or FLC levels do not exclude the development of MM development. Until better molecular markers for progression to MM are available, clinicians have to use clinical measures in combination with routine blood tests (including renal function, hemoglobin, and serum calcium) and serum and urine M-protein markers in their monitoring of MGUS patients. (Adapted from Landgren et al., 2009.45 )
M-protein concentrations year-by-year over time prior to multiple myeloma. Two major patterns of MGUS prior to multiple myeloma: “evolving MGUS” and “non-evolving MGUS.” In about half the study population, the M-protein concentration and involved FLC-ratio levels showed a year-by-year increase prior to MM diagnosis, while the other half maintained largely stable abnormal serum protein levels up to the diagnosis of MM.45 Currently, we do not know if this represents a genetic switch in the tumor cells, a change in the host, or a combination; neither do we know if these different M-protein concentration patterns represent different biology when MM arises. One might speculate that there could be differences in response to therapy and survival. Future studies need to address these and other related questions. On a clinical note, one has to keep in mind that stable M-protein or FLC levels do not exclude the development of MM development. Until better molecular markers for progression to MM are available, clinicians have to use clinical measures in combination with routine blood tests (including renal function, hemoglobin, and serum calcium) and serum and urine M-protein markers in their monitoring of MGUS patients. (Adapted from Landgren et al., 2009.45 )
Another study evaluated 30 MM cases with available prediagnostic serum stored in the U.S. Department of Defense Serum Repository.48 Because this study took advantage of stored samples from individuals who served in the Army, the patients were younger (median age 48 years); 97% were males and 47% were African Americans. Although there were differences between the two studies with regard to the patients' characteristics, the results were very similar. The military study found that 27 of the 30 (90%; 95% confidence interval 73%–98%) MM patients had had a preceding MGUS diagnosis. Of the three patients with no detectable MGUS preceding the diagnosis of MM, one had only one prediagnostic serum sample available more than 5 years before the MM diagnosis and the other two were found to have IgD MM (a MM subtype with very low levels of monoclonal immunoglobulin secretion) with serum samples available only 3 and 5 years before the diagnosis.
This novel observation from two independent studies45,48 establishes an essential role for MGUS in the pathway to MM. Indeed, the finding that MM is consistently preceded by a precursor state is very important in that it emphasizes the scientific need and clinical potential for future studies designed to define high-risk versus low-risk MM precursor disease, and, importantly, to define underlying mechanisms of progression. Ultimately, such insights will identify novel targets that may be used to delay and prevent MM progression.
Need for Better Molecular and Immunophenotypic Markers
On a clinical note, the following is important to keep in mind: while MGUS, SMM, and MM can be differentiated based on clinical diagnostic parameters,28 it is unfortunate that, at this time, there are no definitive molecular or immunophenotypic markers to differentiate the plasma cells of these three different types (Figure 3).49,50 Likewise, none of the known MM genetic abnormalities defined by karyotyping or interphase fluorescence in situ hybridization (FISH) been found to predict progression from MGUS/SMM to MM. Furthermore, two prior FISH-based studies were unable to find any significant cytogenetic differences between MGUS and SMM patients.51,52 Indeed, in 2003, an international workshop reviewed various studies and determined that some cytogenetic anomaly is present in virtually all cases of MGUS and SMM; often these changes cannot differentiate MM from its precursors, although some events, such as p53 deletions and mutations or homozygous deletions of p18, are far more prevalent in highly aggressive, refractory, or extramedullary MM.49,53

The clinical dilemma of smoldering myeloma. (Reprinted with permission from Waxman et al., 2010.43 )
The clinical dilemma of smoldering myeloma. (Reprinted with permission from Waxman et al., 2010.43 )
In research studies designed to uncover myelomagenesis, point-mutation analysis has been valuable. Indeed, it has led to the identification of N-RAS and K-RAS mutations with much higher frequencies in patients with MM compared with MGUS, although they are overrepresented in tumors expressing cyclin D1. This indicates that the second, transformational event may vary depending on the initial oncogenic event.54,55 Interestingly, a case report of five annual FISH studies and genomic microarrays performed on a patient who progressed from SMM to MM found a deletion of chromosomal band 1p23 that was correlated with the transformation.56 While other studies have shown a correlation between a gain of chromosomal band 1q and the development of MM,57,58 this finding may open an avenue for future research in this area. Furthermore, karyotype and FISH in this patient displayed a MYC oncogene translocation in the transition from SMM to MM.56 This has previously been found to occur in 15% of MM cases, but only in 3% to 4% of MGUS/SMM cases.59 In further support, gene-expression profiling has shown that MYC RNA expression is significantly higher in MM versus MGUS versus normal plasma cells.60 Thus, there may be an early increase in MYC expression due to epigenetic factors, followed by a further increase due to chromosomal rearrangements.
Research studies focusing on complex interactions in the bone marrow have been carried out using flow cytometry. As discussed above in the section on the Spanish PETHEMA risk-stratification model, characteristic changes in aberrant plasma cells include absent CD19, lack of CD45, decreased CD38, and/or overexpression of CD56.61 A prior investigation found that almost all cases of MM have ≥95% abnormal plasma cells, compared with 60% and 18% of SMM and MGUS cases, respectively.40 Furthermore, a recent gene-expression profiling analysis of bone marrow endothelial cells found differences in gene-expression patterns between MGUS and MM.62 Differences with regard to cellular and secreted components of the microenvironment have also been observed in MGUS compared with MM patients.63 Conversion from precursor to full-blown disease has been proposed to be related to an “angiogenic switch” resulting from an alteration in the milieu of pro- and anti-angiogenic cytokines allowing for malignant proliferation64–66 . Finally, microRNAs, short, noncoding RNA sequences that modulate many biological processes by pairing with target mRNAs and regulating their expression,67 have been implicated as playing a role in myelomagenesis.68
Based on the above, we currently lack reliable biological markers to either differentiate plasma cells of MGUS, SMM, or MM or to predict progression from MGUS/SMM to MM.49 As discussed above, our current understanding is that progression from precursor to MM is due to both intrinsic changes of plasma cells and the extrinsic influence of bone marrow stromal cells, angiogenesis, and immunologic factors. Malignant transformation is believed to be mediated, at least in part, through antigenic stimulation.69 Much future work is needed to elucidate the role of the microenvironment in the progression from precursor to MM. Studies focusing on the cells of the microenvironment will be challenging, because they require careful sorting of the numerous cell types that reside in the marrow.50 Adding to this complexity, it is likely that alterations in the microenvironment may allow for both enhanced growth of malignant plasma cells and expansion of the overall plasma-cell niche.50 Importantly, due to heterogeneity of plasma-cell neoplasia, there is a great need for future studies based on prospectively collected, paired samples from the same patient. Such efforts will provide insights that are unattainable from studies comparing populations of patients in different disease states at a single point in time.
Summary and Future Directions
From a clinical standpoint, there are emerging data supporting up-front risk stratification and a model for tailored clinical follow-up for MGUS patients. Until we have more reliable biological markers that allow us to predict the individual patient's risk for MM progression, the 2010 IMWG guidelines advocate the application of the Mayo Clinic risk-stratification model to define low-risk versus intermediate-/high-risk MGUS patients.28 The guidelines recommend that SMM patients be considered candidates for chemoprevention trials28 ; however, off-study observation is still the standard in this group.42
From a research perspective, the development of better biologic and molecular markers will improve our understanding of the molecular pathways involved in myelomagenesis.43,50 This will help us not just in understanding the biology of plasma-cell dyscrasia, but also in identifying newer therapeutic targets and novel treatments for these diseases. The recent finding that MM is consistently preceded by a precursor state (MGUS)45,48 has opened an avenue for future research, and highlights the need for upcoming studies based on prospectively collected, paired samples from the same patient with the aim of distinguishing benign (low-risk) from progressive (high-risk) precursor disease and uncovering the underlying mechanisms of progression. Such insights will allow us to define novel targets that can be used to delay and prevent MM progression.43,50
Finally, it is important to consider the clinical implications of recently reported familial aggregation patterns for MGUS and MM.15,17 First-degree relatives of patients with MGUS and MM are at an increased relative risk of MGUS/MM.15,17 However, because of the low baseline risk in the general population (0.2–0.3% of men and women in the United States will develop MM between their 50th and 70th birthdays),70 the absolute risk of a first-degree relative developing MM is still low. At our institution, relatives of MGUS/MM patients are informed that they have a higher relative risk of developing MGUS and MM (compared with family members of unaffected individuals). However; we emphasize that the absolute risk of developing MM is low and, outside of clinical studies, observation is still the standard for MM precursor disease.42 At this time, no therapy has been found to prolong survival for MGUS/SMM patients, so we do not currently recommended screening for plasma-cell diseases among family members outside of clinical research studies.
Disclosures
Conflict-of-interest disclosure: Author declares no competing financial interests.
Off-label drug use: Len/Dex for smoldering myeloma.
Funding: This work was supported by the Intramural Research Program of the National Cancer Institute of the National Institutes of Health.
Correspondence
Dr. Ola Landgren, Multiple Myeloma Section, Medical Oncology Branch, Center for Cancer Research, National Cancer Institute, National Institutes of Health, 9000 Rockville Pike, Bldg 10/Room 13N240, Bethesda, MD, 20892, USA; Phone: 301-496-0670; Fax: 301-402-0172; e-mail: landgreo@mail.nih.gov
