
Abstract
In the early 1980s, adult acute lymphoblastic leukemia (ALL) was a rarely curable disease with overall survival < 10%. After adapting combinations employed by pediatric groups, the outcome improved to 30–40%. A period of stagnation followed with improvement only in distinct subgroups. In the past 5 years, however, striking new developments have been noticeable. Progress has been made in molecular diagnostics of ALL. Improvements to standard therapy including stem cell transplantation (SCT) have occurred and a variety of new drugs for ALL are under evaluation. Rapid diagnosis and classification of ALL is increasingly important to identify prognostic factors and molecular genetic subsets that will be the focus of “targeted” therapies as we enter the era of subset specific treatment. In the following review we will discuss treatment of adult ALL (excluding elderly patients,1 adolescents2 and patients with Ph/BCR-ABL positive ALL3).
Standard Treatment of Adult ALL
In the past decade two basic types of prospective trials have been reported in adult acute lymphoblastic leukemia (ALL) (Table 1 ). One is dedicated to comparative analysis of the role of stem cell transplantation (SCT) with allogeneic SCT in all patients with sibling donors4,5,6,7; the other group consists of studies focused on optimization of chemotherapy with SCT only for subgroups such as Philadelphia chromosome (Ph)-positive ALL8,9 or based on prognostic models.10–14 Complete response (CR) rates ranged between 74% and 93% and the overall survival (OS) between 27% and 48%. No difference is evident for OS of studies focused on SCT (N = 2696), with a weighted mean of 84% for CR and 35% for OS,4–7 and studies with risk-adapted approaches (N = 2443), with mean CR rate of 83% and OS of 36%.10–14,8 Notably, only a few studies included patients aged above 60 years.6,9–11,13
Induction therapy
Standard induction of adult ALL includes at least a gluco-corticoid, vincristine, an anthracycline and probably asparaginase. In response to pediatric results that show a decreased central nervous system (CNS) relapse rate and improved survival,15 prednisone is now being replaced by dexamethasone. The dexamethasone schedule has to be considered carefully since continuous application of higher doses may lead to long-term complications such as avascular bone necrosis15 and to increased morbidity and mortality due to infections. The German Multicenter Study Group (GMALL) observed in their pilot trial 06/99 an early mortality of 16% with dexamethasone 10 mg/m² given on days 1–16 compared to 5% for an interrupted schedule (days 1–5,11–14) with corresponding CR rates of 76% and 82%.16
The most frequently used anthracycline is daunorubicin (DNR). One randomized study showed a disease-free survival of 36% for DNR at 30 mg/m² compared to 30% for idarubicin (9 mg/m²) given weekly in induction.14 Many groups have replaced weekly applications by higher doses of DNR (45–80 mg/m²) on subsequent days. Promising results of smaller trials have not always been reproduced. One possible reason is the increased hematologic toxicity of these sequential daily dosing schedules. The GIMEMA Study Group evaluated a previously published regimen with high-dose anthracylines. The CR rate was 93% and event-free survival 55% in the originally published small population compared to 80% CR and 33% OS in the larger GIMEMA multicenter trial.17 Thus, it remains open whether intensified anthracyclines are beneficial for all subgroups, particularly in terms of molecular remission, and further trials are needed. The up-front application of cyclophosphamide may be of benefit as well,8,18 although this has not been confirmed in a randomized trial.19 The majority of current studies in adult ALL include asparaginase during induction therapy, although total doses are much lower than in pediatric trials. In induction asparaginase is often given parallel to steroids in patients with cytopenia and may induce additional toxicities such as coagulation disorders and hepatopathies, which are not predictable. Asparaginase may thereby lead to treatment delays and compromise dose intensity in individual patients. Supportive care is of increasing importance during induction, including the concomitant application of granulocyte colony-stimulating factor throughout chemotherapy.8,16
Future options for induction therapy
With intensified induction in adult ALL the balance between efficacy and toxicity must be considered. Treatment-related early death occurs in up to 11% of patients and significant morbidity results from the consequences of prolonged cytopenias, such as subsequent infections including fungal pneumonias. These toxicities may compromise further treatment and dose intensity. The advantage of a high CR rate may thereby be outweighed by the inability to proceed with postremission therapy and may also compromise the outcome of subsequent SCT. Whereas a limit for intensification of myelotoxic drugs seems to have been reached, there is still space to intensify non-myelotoxic drugs (Table 2 ).
In the future, an increase of molecular CR rates may be the most important goal and measure for efficacy of induction therapy. Molecular remission may be defined as a level of minimal residual disease (MRD) after induction therapy below the detection limit of clone-specific PCR, which is generally 10−4 (i.e., 0.01% blasts or 1 blast in 10,000 normal cells); the frequency of molecular CR in adult ALL certainly depends on the type of induction therapy, and so far few results are available. CR ranges from 50% for Ph+ ALL treated with imatinib and chemotherapy20 to 60% for standard risk ALL21 and is thereby significantly lower than in pediatric ALL.
Consolidation therapy
Intensive consolidation is standard in the treatment of ALL based on pediatric studies and historic comparisons although randomized trials often failed to demonstrate a benefit of intensification; this may be due to insufficient numbers of patients in these trials.5,19 Consolidation cycles in large studies are very variable and it is impossible to evaluate their individual efficacy. In general, it seems that intensive application of HD methotrexate (MTX) is beneficial. However, in adults dosages are probably limited at 1.5–2 g/m² if given as 24-hour infusion. Otherwise toxicities, particularly mucositis, may lead to subsequent treatment delays and decreased compliance. Toxicity, but also efficacy, may be reduced with a shortened infusion time (e.g., 4 hours). In a pediatric trial for B-cell neoplasias 5 g/m² MTX given as 4-hour infusion was less toxic than a 24-hour infusion, but—at least in high-risk patients—it was associated with poorer outcome.22 The situation may change when improved prophylaxis of mucositis, e.g., with keratinocyte growth factor, becomes available.
Pediatric trials have underlined the important role of dose intensification of ASP. There is also the need for intensification in adult patients, particularly in consolidation, where less toxicity can be expected compared to induction. Several studies have also demonstrated that a modified induction (reinduction) improves outcome. The role of HD anthracylines, podophyllotoxins and HD cytarabine in consolidation remains open, particularly if potential late effects are considered. For future studies, a design with postinduction cycles with new drugs, evaluated by MRD measurement, may be an useful option. Furthermore, in adult ALL stricter adherence to protocols with fewer delays, dose reductions and omission of drugs due to toxicities may be important factors that could result in therapeutic progress (Table 2 ).
Maintenance therapy
Maintenance, even after intensive induction and consolidation, is still standard for ALL patients since all attempts to omit it led to inferior long-term outcome with LFS rates of 18–28%.23 Therefore, some groups even prolong maintenance therapy beyond 2 years of total treatment duration. MTX, preferably given intravenously (I.V.), and mercaptopurine (MP) given orally are the backbone of maintenance. Attempts for intensification by I.V. application of higher doses of MP did not increase efficacy in adults.9 It may be useful to aim for leukocyte counts below 3000/μL during maintenance24 in order to achieve optimal suppression of residual disease. Randomized trials failed to demonstrate an advantage of intensified maintenance with HD cycles.23 However, only a few patients actually received these regimens as scheduled; adults often show poor compliance to intensive maintenance due to toxicities and for social reasons. Therefore, maintenance with less intensive reinforcements, e.g., with vincristine or steroids, may be more feasible; it is still open whether and to what extent maintenance therapy is necessary in ALL subgroups. Patients with mature B-ALL do not require maintenance; in T-ALL, with relapses up to 2 ½ years, it may be less important than in B-precursor ALL, with relapses up to 5 years. Therefore, it is reasonable to test MRD evaluation for decision making on maintenance therapy in prospective studies, as is currently done in the GMALL study group.
Stem cell transplantation
Although the majority of large prospective studies in adult ALL addressed the issue of indications for SCT in first CR, scheduling and procedures are still not adequately standardized. To circumvent the problem with comparisons of SCT vs. chemotherapy, several groups have developed prospective trials with a “genetic” randomization offering allogeneic (allo sib) SCT in CR1 to all patients with a sibling donor. The study results certainly depend on the compared “conventional” treatment approach. Some groups scheduled autologous (auto) SCT only25 and others a randomized comparison of auto SCT and chemotherapy.4,6,14,26
The preferable approach for this trial design is “intent-to-treat” analysis that compares patients with donors to those without donors. The hardest outcome parameter is the OS of the total patient cohort, which answers the question whether an SCT-based treatment concept can improve overall outcome. OS of studies with “genetic randomization” is not superior to chemotherapy studies (see above), which is partly due to the fact that allo sib SCT could be realized in only 11–38% of the patients.4–6,14,25,26 Even if allo sib SCT yielded favorable results, due to infrequent realization the impact on overall outcome is too small.
Donor versus no donor
Chemotherapy versus autologous SCT
In several randomized studies no significant difference was detected.4,6,14,27 The major advantage of auto SCT is probably a shorter total therapy duration. Auto SCT may be of interest in patients with low MRD after induction, MRD negative stem cell graft and the option to give MRD-based maintenance after auto SCT.
Allogeneic sibling versus matched unrelated
According to the recent IMBTR data (www.imbtr.org), the OS after allo sib SCT in patients older than 20 years is 48% compared to 42% for matched unrelated (MUD) SCT. Also, in large prospective trials the results are similar with higher relapse rates for sibling and higher mortality (TRM) for MUD-SCT. The ECOG/MRC study reported an OS of 55% for sibling, 46% for MUD SCT (restricted to Ph/BCR-ABL+ ALL) and 39% for auto SCT.26 In the GMALL study 06/99 the OS was 53% for sibling and 44% for MUD SCT.28 The TRM for allo sib SCT in prospective trials ranged between 15% and 26%4–6,14,25–27 and was higher for MUD-SCT.26 Several factors such as intensity of therapy before SCT, preparative regimens, immunosuppressive therapy after SCT and also the experience and conditions at SCT centers may influence these outcomes. In order to achieve further reduction of TRM in MUD SCT and of relapse rate for allo sib SCT these factors have to be carefully considered.
An evidence-based review29 concluded that SCT in CR1 is recommended in high-risk but not in standard-risk ALL patients. In second CR the outcome of SCT is superior to chemotherapy. Related and unrelated SCT yield comparable results, whereas allo SCT is probably superior to auto SCT. Results of auto SCT are not superior compared to chemotherapy.
Future options in SCT
Larger cooperative studies are urgently required to prospectively evaluate the optimal integration of SCT in front-line therapy. One important point is the balance between efficacy and toxicity of treatment before SCT and preparative regimens in order to reduce TRM. Also, the optimal timing of SCT has to be defined. MRD before and after SCT should be evaluated prospectively in order to identify decision criteria for invention of maintenance therapy and/or immunotherapy such as donor-lymphocyte infusions.
CNS prophylaxis
Prophylaxis of CNS relapse seems to be no longer a significant problem in adult ALL. In protocols with intensive intrathecal (i.th.) therapy and systemic HD therapy, the rate is below 5%. Some trials including GMALL rely on CNS irradiation.4,10,11,14 Risk factors for CNS disease such as elevated WBC or LDH, traumatic lumbar punctures and phenotypes as mature B-ALL and T-ALL are well known. Therefore, risk-adapted approaches to prophylaxis seem to be reasonable.9 It should be kept in mind, however, that effective CNS prophylaxis not only reduces the risk of isolated CNS relapse but also improves general outcome. De-escalation of CNS prophylaxis should therefore be done carefully. In the future the use of liposomal cytarabine for i.th. therapy may help to reduce the number of i.th. applications, and thereby the risk of contamination, and improve efficacy with the aim to replace CNS irradiation in defined populations.
Prognostic Factors and Relevant Subgroups in Adult ALL
Age
Age is probably the most important prognostic factor.24 OS continuously decreases with increasing age from 34–57% below 30 years to 15–17% above 50 years.5,7–9,19 Some groups defined age above 30–35 years as indication for SCT in CR1.27 This is probably counterproductive, since the outcome of SCT also significantly decreases with age.26
White blood cell count
An elevated WBC at diagnosis (> 30, 50 or 100,000/μL) is associated with a higher relapse risk.4,5,9,19 In the GMALL studies WBC > 30,000/μL in B-precursor ALL (c-/pre-BALL) was even considered as the most deleterious prognostic factor with OS of 19–29%,7,11 whereas in T-ALL WBC was not a significant factor in a GMALL multivariate analysis.11 Furthermore, high WBC may be associated with the risk of complications during induction and with an increased risk of CNS relapse. The biological reason for the highly resistant behavior of B-precursor ALL with high WBC is unclear. In the GMALL studies these patients show a high relapse rate but also seem to have a higher mortality with chemotherapy and SCT.28 In these patients, evaluation of MRD, use of experimental drugs and SCT in CR1 modalities may be particularly important.
Immunophenotype
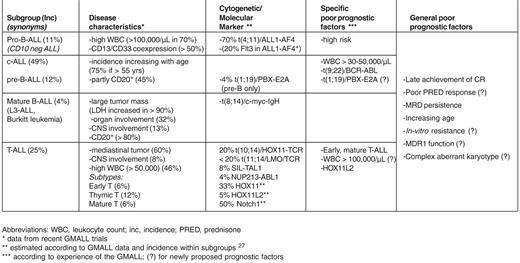
A complete immunologic characterization at diagnosis is required to identify subtypes with different presentations and prognoses, distinct cytogenetic and/or molecular aberrations, surface markers as potential targets for antibody therapy and targets for other innovative therapies (Table 3 ). Pro-B–ALL and/or t(4;11)+ ALL is considered a poor prognostic subgroup in many trials. It appears to be particularly susceptible to SCT.23 In the ongoing GMALL studies, pro-B–ALL is considered an indication for SCT in CR1. The survival was 74% for allo sibling SCT in CR1, indicating that pro-B–ALL has the most favorable outcome after SCT compared to other ALL subgroups.28Common (c)/pre-B–ALL bears a large proportion of Ph/BCR-ABL+ ALL, which will be discussed separately. Some groups consider the translocation t(1;19), which occurs in pre-B–ALL, an unfavorable feature.14,25 Since the prognostic impact depends on the treatment regimen and the aberration is very rare (< 3% incidence), convincing data are rare—as for many other cytogenetic aberrations—and there is no general agreement on its role as a prognostic factor. c/pre-B–ALL can be subdivided into standard- and a high-risk group with significantly different outcome (Table 3 ). However, even in standard risk B-lineage ALL the outcome is not satisfactory, and this is a major reason for slow improvement of overall results in adult ALL. Mature B-ALL is treated according to different concepts (see below).
Many groups have confirmed the superior outcome of T-lineage ALL compared to B-lineage.7,11 T-ALL comprises the subtypes early T-ALL, thymic (cortical T-ALL CD1a pos) and mature T-ALL. Within T-ALL, subtype was the most significant prognostic factor in the GMALL studies. The LFS was significantly poorer for early T-ALL (25%) and mature T-ALL (28%) compared to thymic T-ALL (63%).11 Therefore, the former subgroups are considered as indications for SCT in CR1 in the GMALL studies. Interim results showed that outcome can thereby be improved.28
The biologic importance of immunologic subtype within T-ALL was underscored by the fact that elevated expression of HOX11, HOX11L2, SIL-TAL1 and CALM-AF10 is associated with subtypes, i.e., maturation states of thymocytes (reviewed in 30). Other groups observed inferior outcomes for early T-ALL,31,32 coexpression of CD13, CD33 and/or CD34,31 HOX11L2 and SIL-TAL+ T-ALL.32 Overexpression of HOX11, which is associated with thymic T-ALL, may confer a favorable prognosis. Notch1 activating mutations with as yet unclear prognostic relevance were identified in up to 50% of T-ALL cases.30 They may be targeted by γ-secretase inhibitors. Four percent of TALL show the NUP214-ABL1 aberration which may identify a target population for imatinib therapy. With current treatment regimens, CR rates of more than 80% and a LFS above 50% can be achieved in T-ALL.
Interestingly, outcome after SCT also appears to be influenced by immunophenotypes. In the GMALL studies the most favorable OS after SCT was achieved for pro-BALL and early T-ALL whereas it was poorest in c/pre-BALL with high WBC.28
Treatment response and minimal residual disease
Beside age the most relevant prognostic factor in ALL is the achievement of CR, as underlined by the favorable outcome in children.19 Further prognostic factors related to treatment response are delayed time to CR or response to prednisone therapy. A more accurate approach to assess individual response is minimal residual disease (MRD) evaluation24,23 since this is an independent prognostic factor that reflects primary drug resistance as well as individual realization of therapy and unknown host factors.
Two major aims were followed with longitudinal MRD evaluation in adult ALL. The first was to identify patients with high risk of relapse as candidates for treatment intensification with SCT or experimental therapy. In general, the decrease of MRD occurs more slowly in adults, and fewer patients reach a negative status.33 Decision making immediately after induction is therefore too early. However, after start of consolidation, high MRD (> 10−4) at any time-point is associated with a high relapse risk of 66–88%,21 and the predictive value increases at later time-points (months 6–9).33 In the GMALL studies patients, with high MRD (> 10−4) after induction and first consolidation are identified as high risk and are candidates for SCT in CR1.34
The second aim, to identify patients with low risk of relapse in whom treatment reduction may be justified, is more difficult to reach. An early and rapid decrease of MRD during induction is associated with a relapse risk of only 8%.21 However, this is observed in only 10% of the adult patients. In the GMALL studies, patients with negative MRD status after induction, which is repeatedly confirmed during the first year and measured with two sensitive markers, are considered as MRD low risk. Thirty percent of the patients fulfill these criteria.
MRD evaluation furthermore offers the option of assessing molecular CR and thereby evaluating different induction therapies and detecting molecular relapses. These are two important new items for follow-up analysis in adult ALL. Even in some phase II studies, “molecular relapse” is already an inclusion criterion. This makes sense since patients with increase of MRD above 10−4 after achievement of molecular CR are at high risk of relapse (> 80%) and therapeutic action should be taken.
MRD evaluation has certain limitations. The technical procedure is time consuming and expensive and requires highly specialized staff. The predictive value depends on the technical quality such as sensitivity (10−4), number of targets (at least two for immunoglobulin or TCR-rearrangements) and on the frequency of evaluations (3 monthly). At least in multicenter studies these prerequisites can often not be fulfilled. Sensitivity of MRD-evaluation, with the exception of BCR-ABL–based analysis, is also not sufficient to evaluate the efficacy of consolidation cycles since in most patients MRD is then below the detection limit.
New integrated risk classification
A variety of “molecular” markers newly detected by microarray analysis have been proposed as prognostic factors.35 Other “clinical” factors such as obesity, underweight, or even female gender have been proposed as high-risk features in different studies.7,31 Certainly the prognostic relevance of new “clinical” or “molecular” prognostic factors also depends on the applied treatment regimen. Therefore, and also to keep risk stratification practicable, the integration of new prognostic factors in risk models has to be done carefully, particularly because risk factors generally lead to the indication of SCT in CR1 with considerable morbidity and mortality. However, molecular aberrations with prognostic relevance may stimulate the analysis of underlying mechanisms and possible new drug targets.
Overall Treatment Strategies in Adult ALL
Treatment of adult ALL is becoming more complicated, due to the increasing tendency to treat based on biologic risk group. Treatment approach also depends on factors unrelated to the disease biology such as the availability of a stem cell donor, co-morbid conditions, treatment response and availability of targeted drugs (Figure 1 ). Prognostic factors and patient characteristics therefore no longer serve only for identification of candidates for SCT in first CR but to define individualized treatment approaches (examples of which are discussed below).
Subgroup-adjusted treatment
The best example is probably mature B-ALL and Burkitt’s lymphoma, which is generally treated in separate studies with short intensive cycles, leading to improvement in OS rate from < 10% to > 50%. Since B-ALL shows CD20 expression in > 80% of the cases treatment was further refined by integration of anti-CD20 before each chemotherapy cycle with very promising results of 70–80% OS in preliminary analyses.36,37
Age-adapted treatment
Individualized treatment
According to MRD
The approaches to integrate MRD analysis in prospective risk stratification of adults can be different in terms of (1) time-point; (2) selection of patients for MRD risk stratification; (3) combination of MRD-based and conventional-risk factors; and (4) MRD-based treatment decisions. It is hardly possible to identify adult low-risk patients in whom reduction of therapy would be justified. In the GMALL study these patients are defined according to very strict criteria (see above) in order to omit maintenance therapy. Even so, 20–30% of these patients relapse. The major aim of MRD-based studies is to identify patients with high risk of relapse for treatment intensification by SCT since very few adults are candidates for “de-escalation” of therapy. It remains to be demonstrated that this is an effective strategy, since patients with high MRD before SCT have an increased risk of relapse and could probably benefit from additional conventional (even experimental) therapy to reduce tumor load. On the other hand, it has to be questioned whether patients who are candidates for SCT based on conventional or molecular risk factors should receive allo SCT if they are MRD negative. Thus, the best strategy is not yet known and must be tested prospectively.
According to drug resistance
Expression of MDR-1 (multidrug resistance gene 1) has been associated with a poorer prognosis in ALL.17,31 Also, in-vitro sensitvity testing was able to identify patients with resistance to conventional cytostatic drugs which was associated with an inferior prognosis. More recently it was demonstrated that in-vitro resistance is associated with distinct gene expression profiles.38In-vitro resistance testing is also increasingly used for preclinical effectivity testing of potential new cytostatic drugs. In the future it may be possible to predict response to induction regimens to adapt therapy to individual susceptibility.
Risk-adapted indications for SCT
There is no general agreement on indications for SCT in first CR, but until results of the ECOG/MRC study are available the evidence is in favor of risk-adapted approaches.29 SCT indications have to keep the balance between the expected reduced relapse risk and increased mortality. Also, late effects are more pronounced in SCT patients, the quality of life seems to be poorer and the risk of rapid procedure-related death is 20–30% compared to chemotherapy with more prolonged risks. SCT in CR1 from sibling or unrelated donor seems to be justified in subgroups of ALL with OS below 40% with chemotherapy and should probably not be offered to patients with OS above 50%. These outcomes clearly depend on the different chemotherapy regimens. The role of auto SCT remains to be determined in optimized schedules. For older high-risk patients and those with contraindications for conventional SCT, nonmyeloablative SCT may be a reasonable alternative to be studied in prospective trials with an expected LFS of 34% if performed in first CR.39
Targeted therapies
Ph/BCR-ABL+ ALL
New molecular therapeutic strategies with imatinib and other new kinase inhibitors led to a considerable improvement of this formerly most unfavorable subgroup. These issues were discussed extensively elsewhere.3
Antibody therapy
ALL blast cells express a variety of specific antigens such as CD20, CD19, CD22, CD33, CD52 that may serve as targets for treatment with monoclonal antibodies (MoAb). MoAb therapy is an attractive treatment approach in ALL since it is targeted, subtype-specific, and has different mechanisms of action and side effects than chemotherapy. Application may be most promising in the setting of MRD. The anti-CD20 antibody has been successfully integrated in therapy of mature B-ALL. It has also been explored in several pilot studies for CD20+ B-precursor ALL. In a GMALL protocol for elderly patients, rituximab was added before chemotherapy cycles starting from induction for a total of 8 applications. The combination of hyper-CVAD regimen with rituximab in B-precursor ALL was feasible, and a favorable outcome of CD20+ ALL was reported (reviewed in 40). Several studies with anti-CD52, either in relapse or in a state of MRD, are ongoing. The CALGB has integrated anti-CD52 as consolidation in front-line therapy and demonstrated feasibility in a dose-finding study. Efficacy data are not yet available.41 Further antibodies are summarized in Table 4 .
Targeted therapy in T-ALL
Several new options for targeted therapy for T-ALL (Table 4 ) are forthcoming and, based on results in phase I-II studies, it will be necessary to define priorities. Thus, the purine analogue Nelarabine could be soon integrated in prospective trials of front-line therapy as consolidation cycle. Other drugs, such as Forodesine, a purine nucleoside phosphorylase inhibitor, may be useful during maintenance therapy if efficacy is proven.
Evaluation of new cytostatic drugs
Advances in the understanding of molecular mechanisms of disease, the successful model of imatinib and the increasing interest of pharmaceutical companies in orphan diseases has led to the development of several new therapeutic approaches for ALL (Table 4 ). For some of them, early clinical data are becoming available and many of these drugs fit in subtype adjusted, targeted therapies. Evidence-based priorities for clinical evaluation in relapsed ALL and for integration in front-line therapy have to be defined that take the number of targets and drugs into account.
Future Risk Stratification and Treatment Concepts for Adult ALL
Risk and subtype adjusted treatment strategies led to considerable improvement of outcome in mature B-ALL, TALL and Ph+ ALL, but to a lesser extent in adult patients with B-precursor ALL. Future concepts will integrate a variety of additional factors, thereby resulting in a more complex, flexible and patient specific treatment approach (Figure 1 ). In addition to these sophisticated approaches a better adherence to protocols, support of patients to improve their compliance and documentation of compliance are warranted in adult ALL. Treatment should be done at experienced centers only and closer cooperation between internal medicine and pediatrics, including cooperative studies, would be desirable.
The design of prospective trials will be challenging since they will focus even more on smaller subgroups of ALL and window studies with new drugs. These trials will only be possible in larger, international study groups that are able to recruit sufficient patient numbers. In Europe an important step toward this goal was made by the foundation of a European Working Group for Adult ALL (EWALL).42 In order to enable any intergroup comparison, international efforts similar to those undertaken in childhood ALL are required to define uniform criteria for diagnostic classification, definition of subgroups and even prognostic factors.
Results of large trials in adult acute lymphoblastic leukemia (ALL).*
| Study | Year | N | Median Age (Range) | SCT | CR Rate | Early Death | Survival |
|---|---|---|---|---|---|---|---|
| Abbreviations: Ph+, SCT in Philadelphia chromosome–positive ALL; PO, prospective SCT in all pts with donor; PR, SCT according to prospective risk model; HR, prospective SCT in a study for HR patients only; n.r. not reported. | |||||||
| * Survival of CR patients | |||||||
| CALGB 9111, USA5 | 1998 | 198 | 35 (16–83) | Ph+ | 85% | 8% | 40% (3 y) |
| LALA 87, France1 | 2000 | 572 | 33 (15–60) | PO | 76% | 9% | 27% (10 y) |
| NILG 08/96, Italy7 | 2001 | 121 | 35 (15–74) | PR | 84% | 8% | 48% (5 y) |
| GMALL 05/93, Germany8 | 2001 | 1163 | 35 (15–65) | PR | 83% | n.r. | 35% (5 y) |
| JALSG-ALL93, Japan2 | 2002 | 263 | 31 (15–59) | PO | 78% | 6% | 30% (6 y) |
| UCLA, USA9 | 2002 | 84 | 27 (16–59) | PR | 93% | 1% | 47% (5 y) |
| Sweden10 | 2002 | 153 | 42 (16–82) | PR | 75% | n.r. | 28% (5 y) |
| GIMEMA 0288, Italy12 | 2002 | 767 | 28 (12–60) | — | 82% | 11% | 27% (9 y) |
| MD Anderson, USA6 | 2004 | 288 | 40 (15–92) | Ph+ | 92% | 5% | 38% (5 y) |
| EORTC ALL-3, Europe3 | 2004 | 340 | 33 (14–79) | PO | 74% | n.r. | 36%*(6 y) |
| LALA 94, France11 | 2004 | 922 | 33 (15–55) | PR | 84% | 5% | 36% (5 y) |
| GOELAL02, France13 | 2004 | 198 | 33 (15–59) | HR | 86% | 2% | 41% (6 y) |
| MRC XII/ECOG E 2993, UK-USA4 | 2005 | 1521 | 15–59 | PO | 91% | n.r. | 38% (5 y) |
| GIMEMA 0496, Italy14 | 2005 | 450 | 16–60 | n.r. | 80% | n.r. | 33% (5 y) |
| Pethema ALL-93, Spain15 | 2005 | 222 | 27 (15–50) | HR | 82% | 6% | 34% (5 y) |
| Weighted mean | 7262 | 84% | 7% | 35% | |||
| Study | Year | N | Median Age (Range) | SCT | CR Rate | Early Death | Survival |
|---|---|---|---|---|---|---|---|
| Abbreviations: Ph+, SCT in Philadelphia chromosome–positive ALL; PO, prospective SCT in all pts with donor; PR, SCT according to prospective risk model; HR, prospective SCT in a study for HR patients only; n.r. not reported. | |||||||
| * Survival of CR patients | |||||||
| CALGB 9111, USA5 | 1998 | 198 | 35 (16–83) | Ph+ | 85% | 8% | 40% (3 y) |
| LALA 87, France1 | 2000 | 572 | 33 (15–60) | PO | 76% | 9% | 27% (10 y) |
| NILG 08/96, Italy7 | 2001 | 121 | 35 (15–74) | PR | 84% | 8% | 48% (5 y) |
| GMALL 05/93, Germany8 | 2001 | 1163 | 35 (15–65) | PR | 83% | n.r. | 35% (5 y) |
| JALSG-ALL93, Japan2 | 2002 | 263 | 31 (15–59) | PO | 78% | 6% | 30% (6 y) |
| UCLA, USA9 | 2002 | 84 | 27 (16–59) | PR | 93% | 1% | 47% (5 y) |
| Sweden10 | 2002 | 153 | 42 (16–82) | PR | 75% | n.r. | 28% (5 y) |
| GIMEMA 0288, Italy12 | 2002 | 767 | 28 (12–60) | — | 82% | 11% | 27% (9 y) |
| MD Anderson, USA6 | 2004 | 288 | 40 (15–92) | Ph+ | 92% | 5% | 38% (5 y) |
| EORTC ALL-3, Europe3 | 2004 | 340 | 33 (14–79) | PO | 74% | n.r. | 36%*(6 y) |
| LALA 94, France11 | 2004 | 922 | 33 (15–55) | PR | 84% | 5% | 36% (5 y) |
| GOELAL02, France13 | 2004 | 198 | 33 (15–59) | HR | 86% | 2% | 41% (6 y) |
| MRC XII/ECOG E 2993, UK-USA4 | 2005 | 1521 | 15–59 | PO | 91% | n.r. | 38% (5 y) |
| GIMEMA 0496, Italy14 | 2005 | 450 | 16–60 | n.r. | 80% | n.r. | 33% (5 y) |
| Pethema ALL-93, Spain15 | 2005 | 222 | 27 (15–50) | HR | 82% | 6% | 34% (5 y) |
| Weighted mean | 7262 | 84% | 7% | 35% | |||
Options for improvement of induction and consolidation therapy in acute lymphoblastic leukemia (ALL).
|
Induction
|
Consolidation and maintenance
|
Both
|
|
Induction
|
Consolidation and maintenance
|
Both
|
| Drug | Mechanism of action | Subgroup | Evidence inALL |
|---|---|---|---|
| Abbreviations: B-lin, B-lineage; T-lin, T-lineage; n.s., not specified so far; PNP, purine nucleoside phosphorylase inhibitor | |||
| Monoclonal antibodies | |||
| Rituximab | antiCD20 | B-lin | Trials de novo ALL |
| Alemtuzumab | antiCD52 | B-/T-lin | Trials de novo ALL |
| Gemtuzumab | antiCD33 | CD33+ e.g., early T, pro B | Case reports |
| Epratuzumab | antiCD22 | B-lin | |
| Trastuzumab | Anti-HER2 | n.s. | |
| Cytostatic drugs | |||
| Clofarabine | Purine analogue | n.s. | Phase I-II trials |
| Nelarabine | Purine analogue | T-lin | Phase I-II trials |
| Forodesine | PNP | T-lin (B-Lin ?) | Phase I-II trials |
| Liposomal preparations | |||
| I.th. Cytarabine | Prolonged action | CNS involvement | Trials relapsed ALL |
| Daunorubicine | Less cardiotoxicity (?) | n.s. | Trials relapsed ALL |
| Vincristine | Less neurotoxicity (?) | n.s. | |
| Kinase inhibitors | |||
| Imatinib | Abl tyrosine kinase | Ph/BCR-ABL+ | Trials de novo ALL |
| Dasatinib | Abl-Src kinase inhibitor | Ph/BCR-ABL+ | Phase I-II trials |
| Nilotinib | Abl-kinase inhibitor | Ph/BCR-ABL+ | Phase I-II trials |
| Other | |||
| Tipifarnib | Farnesyl-transferase inhibitor | (T-ALL ?) | |
| LY450139, MK0752 | γ-Secretase inhibitor | Notch1 aberrant T-ALL | Phase I-II trials |
| Rapamycin and other | mTOR inhibitor | n.s. | |
| PKC412 and other | FLT3 inhibitor | MLL rearranged | |
| Drug | Mechanism of action | Subgroup | Evidence inALL |
|---|---|---|---|
| Abbreviations: B-lin, B-lineage; T-lin, T-lineage; n.s., not specified so far; PNP, purine nucleoside phosphorylase inhibitor | |||
| Monoclonal antibodies | |||
| Rituximab | antiCD20 | B-lin | Trials de novo ALL |
| Alemtuzumab | antiCD52 | B-/T-lin | Trials de novo ALL |
| Gemtuzumab | antiCD33 | CD33+ e.g., early T, pro B | Case reports |
| Epratuzumab | antiCD22 | B-lin | |
| Trastuzumab | Anti-HER2 | n.s. | |
| Cytostatic drugs | |||
| Clofarabine | Purine analogue | n.s. | Phase I-II trials |
| Nelarabine | Purine analogue | T-lin | Phase I-II trials |
| Forodesine | PNP | T-lin (B-Lin ?) | Phase I-II trials |
| Liposomal preparations | |||
| I.th. Cytarabine | Prolonged action | CNS involvement | Trials relapsed ALL |
| Daunorubicine | Less cardiotoxicity (?) | n.s. | Trials relapsed ALL |
| Vincristine | Less neurotoxicity (?) | n.s. | |
| Kinase inhibitors | |||
| Imatinib | Abl tyrosine kinase | Ph/BCR-ABL+ | Trials de novo ALL |
| Dasatinib | Abl-Src kinase inhibitor | Ph/BCR-ABL+ | Phase I-II trials |
| Nilotinib | Abl-kinase inhibitor | Ph/BCR-ABL+ | Phase I-II trials |
| Other | |||
| Tipifarnib | Farnesyl-transferase inhibitor | (T-ALL ?) | |
| LY450139, MK0752 | γ-Secretase inhibitor | Notch1 aberrant T-ALL | Phase I-II trials |
| Rapamycin and other | mTOR inhibitor | n.s. | |
| PKC412 and other | FLT3 inhibitor | MLL rearranged | |

Course of therapy in adult acute lymphoblastic leukemia and potential influencing factors.
Course of therapy in adult acute lymphoblastic leukemia and potential influencing factors.
