Abstract
Since the introduction of tyrosine kinase inhibitors (TKIs) at the beginning of the millennium, the outlook for patients with chronic myeloid leukemia (CML) has improved remarkably. As such, the question of life expectancy and survival has become less problematic while quality of life and family planning have become more so. While TKIs are the cornerstone of CML management, their teratogenicity renders them contraindicated during pregnancy. In recent years, patients who satisfy standardized criteria can stop TKI therapy altogether, and indeed, in eligible patients who wish to become pregnant, these objectives overlap. However, not all patients satisfy these criteria. Some pregnancies are unplanned, and a number of patients are pregnant when diagnosed with CML. In these patients the way forward is less clear, and there remains a paucity of good evidence available to guide treatment. In this article, we summarize the relevant literature and provide a framework for clinicians faced with the challenge of managing CML and pregnancy.
Learning Objectives
Manage CML diagnosed in pregnancy
Manage established CML in unplanned pregnancies
Facilitate planned childbirth in established CML
CLINICAL CASE
A 35-year-old woman was diagnosed with chronic myeloid leukemia (CML) in chronic phase in 2014. There were no additional chromosomal abnormalities, and the European Treatment and Outcome Study (EUTOS) long-term survival score was intermediate. She was started on imatinib and achieved complete cytogenetic remission (CCyR) at 12 months but was not in major molecular remission (MMR) at 2 years. She has no children but indicates that having a child is very important to her.
Introduction
Targeted tyrosine kinase inhibitors (TKIs) have revolutionized the course of CML. An individual diagnosed with CML, previously a fatal disease, now has an excellent chance of a normal life expectancy.1 Furthermore, for many patients the aim is to achieve deep and sustained molecular responses so that TKI therapy can be discontinued indefinitely.
In Western countries the median age at diagnosis is 57 to 60 years, so many patients are women of childbearing age.2 This is even more relevant in emerging nations, where the median age at diagnosis is 30 to 40 years.3 Before the advent of TKIs, pregnancy and CML were largely incompatible, but the ability to induce profound responses and an increasing prevalence in young patients mean that family planning is an increasingly important discussion topic. There are now 6 TKIs in clinical practice and well- defined sets of hematological, cytogenetic, and molecular landmarks to guide management.4 All produce excellent responses in the majority, but their teratogenicity hinders their use in pregnancy.
This therefore poses a therapeutic and ethical dilemma for the clinician and patient, and decisions must be made with the disease, mother, and fetus in mind. Poorly controlled CML in pregnancy can lead to adverse outcomes for both parties. Persistently raised white blood cell (WBC) counts can result in leukastasis, which may subsequently result in placental insufficiency, intrauterine growth retardation, or fetal mortality.5 Thus, 2 equally important considerations must be balanced: (1) adequately controlling the disease to avoid progression, and (2) minimizing exposure of the fetus to potentially harmful systemic medications.
Despite increasing attention over the last decade, standardized guidance for the management of CML in pregnancy is lacking. Appropriately stratifying patients by disease status at diagnosis and the risk of relapse/progression is helpful when approaching management. They can be generally defined by the following:
- a)
CML diagnosed during pregnancy
- b)
Established CML when the patient is a candidate for treatment- free remission (TFR)
- c)
Established CML when the patient is not a candidate for TFR
CML diagnosed during pregnancy
A diagnosis of CML during pregnancy is not an uncommon occurrence; approximately 10% of pregnancy-related leukemias are CML, and 20% of pregnancy-related CML is in patients diagnosed during pregnancy.6,7 Unsurprisingly, patients often meet the delivery of such grave news at this time with profound shock and anxiety surrounding their own health and that of the unborn child. For the clinician, it is important to be empathic, sensitive, and to draw upon the multifaceted skill set of the surrounding health care team, including but not limited to obstetricians, specialist nurses, psychologists, and therapists.
At diagnosis there are 3 three main aspects to consider, which guide treatment decisions: disease phase, disease burden and time to delivery. If the patient is presenting in blast crisis or chronic phase with multiple high-risk features, serious consideration should be given to termination of the pregnancy in order to commence treatment. Blast crisis is now increasingly rare, but the outlook remains bleak, with median survivals around 12 months.8 Fortunately, the vast majority present in the chronic phase. Upon first consultation, a full outline of the treatment options, the associated risks, and an expected pregnancy road map should be discussed with the patient.
In addition to isolated case reports, 2 studies provided data on multiple patients presenting with CML in pregnancy (Table 1). Assi et al described 15 patients, the majority of whom achieved at least MMR following the start of TKIs.9 One patient who was managed with interferon alfa (IFN-α) during pregnancy was resistant to dasatinib, progressed to blast crisis, and died. Chelysheva et al presented 48 patients, of which 33 went to term.10 Imatinib was given in 13 cases at a median of 18 weeks' gestation (range, 16-35). No congenital abnormalities occurred, but the mothers of 6 of 7 infants born with low birth weights had received imatinib. Two patients demonstrated resistance to multiple TKIs and died secondary to blast crisis. At our center we managed 11 cases of CML diagnosed during pregnancy (Table 2). All patients were alive at last follow-up.
Many patients diagnosed in pregnancy present with manageable cell counts and low-risk disease such that a “watch and wait” strategy is a completely reasonable approach. For patients with rapidly rising WBC counts and/or troublesome symptoms, we discuss below the various options for treatment. Pregnancy itself does not alter the disease course of CML, with the caveat that the true effect of treatment delay on long-term disease control is uncertain.11
TKIs should be avoided in pregnancy, particularly during the first trimester, when the majority of organogenesis occurs, and the fetus is most sensitive to maternal systemic medications.12 In both clinical and preclinical studies, the most commonly observed abnormalities in fetuses exposed to TKIs are bony skull defects and exomphalos.13 Significant “off-target” inhibition, most probably of platelet-derived growth factor receptor alpha, is likely responsible for these malformations.14 Pye et al reviewed the largest cohort to date of 125 patients treated with imatinib during pregnancy, with 103 exposed in the first trimester. Fifty percent of the pregnancies resulted in live births, and 12 fetal malformations were observed. Moreover, the similarity of rare malformations in 3 infants suggests that they were drug induced.13 These findings were corroborated by Abruzzese et al, who concluded that although the majority of pregnancies exposed to imatinib result in normal live births, there is a significant risk of fetal abnormality.15 Dasatinib exhibits the highest incidence of fetal abnormalities and should not be used at any point during pregnancy.16 Nilotinib should not be used in the first trimester, and the sparsity of evidence for bosutinib currently supports avoidance throughout pregnancy.17,18 There have been no published reports on the effect of the newest-generation TKIs, ponatinib and asciminib, on human pregnancy outcomes; however; both demonstrated embryo-fetal toxicity in preclinical studies (Ariad and Novartis investigator brochures, respectively).
While there is no doubt that TKIs should be avoided in the first trimester, there is growing evidence of their safety when used in later pregnancy. The pregnancy registry of the European LeukemiaNet described 41 women who started on a TKI late in gestation (imatinib = 33, nilotinib = 8), and while a small number had malformations, these were deemed unrelated to the TKI by the treating physicians.19 Abruzzese and colleagues confirmed these findings and reported pregnancies in 17 patients, 3 of whom started a TKI during pregnancy (imatinib = 1, nilotinib = 2). All 3 pregnancies resulted in live healthy infants.20 Therefore, when necessary in those with rapidly increasing BCR-ABL1 transcripts, we recommend consideration of TKIs in later pregnancy (second or third trimester). Patients should be aware of the manufacturer's advice to avoid TKIs during pregnancy as well as the potential risks to starting or delaying TKI therapy.
A crucial factor in avoiding complications is the management of thrombocytosis and leukocytosis. Those with significant thrombocytosis should start low-dose aspirin (75-100 mg) and low-molecular-weight heparin, both of which are considered safe in pregnancy, to reduce the risk of thrombosis.21,22 While there is no evidence of a threshold for starting antithrombotic drugs, recent expert recommendations suggest initiation when the platelets exceed 600 × 109/L.7 Clearly, the benefits of avoiding thrombosis must be carefully balanced against the risk of pregnancy-related bleeding. There is little evidence to suggest the best time to stop treatment prior to labor, and the decision is ultimately led by the obstetrician based on the expected mode of delivery and associated procedures.
There are a number of reports of safe hydroxycarbamide (HC) use during pregnancy, albeit mostly in myeloproliferative neoplasms.23,24 The National Toxicology Program gathered information from 33 patients exposed to HC during pregnancy. They reported major malformations in 8% of those exposed to HC in the first trimester and 14% in the second and/or third trimester. Two stillbirths were noted.25 In the recent expert recommendations, HC was not recommended for use during pregnancy.7
Leukapheresis is effective in controlling high WBC counts and can be used safely in pregnancy.26,27 It is, however, not without drawbacks, including availability, cost, and potential problems with repeated intravenous access with risks of infection and bleeding. Our personal practice is to commence leukapheresis when the WBC count is higher than 100 × 109/L.
IFN-α is the only therapeutic option that exhibits anticancer properties and is safe to use throughout pregnancy.28,29 Polyethylene glycol (PEG)–IFN-α is more commonly used now due to its faster and longer-lasting treatment response. Initially, PEG–IFN-α was contraindicated in pregnancy due to concerns around the preservative. Multiple case reports from patients with myeloproliferative neoplasms and viral hepatitis and experience from our own center have not demonstrated any harmful effects.30 The ability of IFN-α to produce meaningful disease control over the remaining period of gestation is variable, and it is associated with unpleasant side effects such as pyrexia and myalgia.31
TKI therapy should begin as soon as possible after pregnancy has concluded. Imatinib and nilotinib are present in breast milk, but the effects of these low drug concentrations on a developing infant are unknown.32-36 There is little information on whether the other TKIs are present in breast milk, but it is safer to avoid their use when breastfeeding. Many women wish to breastfeed, but the decision to delay effective therapy in order to facilitate this must be on a case-by-case basis after a thorough discussion of the risks involved.
It is clear that a “one-size-fits-all” approach is not possible, and treatment should be tailored based on the patient's personal, cultural, and religious wishes. A multidisciplinary approach is paramount. A treatment-free first trimester is the objective, with management in the second and third trimesters remaining largely the same, with reassurance that any treatment administered has a lower risk of causing fetal abnormalities. TKI therapy should be avoided during breastfeeding, but if the mother is insistent, then it should be limited to 2 to 3 weeks to minimize the risk of disease progression.
Established CML: patient is a candidate for TFR
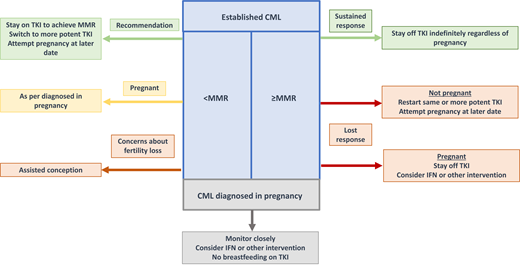
Regardless of pregnancy, a number of patients are eligible for trials of treatment discontinuation. Indeed, the numerous trials of treatment discontinuation in nonpregnant patients can guide management of the pregnant population. Stopping TKIs offers myriad benefits, including a resolution of side effects and a reduction in health care costs and the risk of fetal abnormalities in those attempting pregnancy. Guidelines indicate that patients in the chronic phase who have been on first- or second-line (intolerance only) TKIs for over 5 years and have sustained deep molecular remission for more than 2 years are eligible for treatment discontinuation.4,37 Approximately 50% subsequently lose their MMR, requiring TKI resumption, 80% of which occurs within 4 to 6 months.38,39 Women who wish to become pregnant who are TFR eligible are the most straightforward because they can be managed similarly to their nonpregnant counterparts.4 Assi et al reported planned pregnancies in 7 patients, 6 of whom had a sustained MR4.5 for at least 18 months.9 Five of these patients sustained at least an MMR throughout pregnancy. The 1 remaining patient rapidly lost the response after stopping dasatinib prior to conception but, reassuringly, regained MR4 6 months after restarting.
TKIs can be discontinued and the patient monitored for increases in transcript levels at 4-to-6-week intervals: a patient remaining in MMR can stay off treatment indefinitely, regardless of pregnancy. In the event of MMR loss, management depends on whether the woman is pregnant. If she is not, then she should resume her original or a more potent TKI and reestablish a deep response, with the possibility of attempting pregnancy in the future. This of course depends on individual circumstances, including, importantly, her age. If this is a consideration, then various possibilities can be considered, including referral for oocyte, ovarian, or embryo storage. If she is pregnant, then management depends on the level of tumor burden. Many women reach the end of their pregnancy without losing CCyR or complete hematological remission (CHR) and do not require treatment. If intervention is necessary, then the choices are identical to those for women presenting in pregnancy.
Established CML: patient is not a candidate for TFR
This is the majority of women who represent a spectrum of scenarios ranging from planned pregnancies in those with minimal TKI exposure and a lack of adequate response, to those on long-term treatment who have sustained MMR without satisfying TFR criteria, to those who conceive while on TKI. The evidence for TKI discontinuation in the non-TFR population is growing and shows that conception and pregnancy can be safely navigated. In order to appropriately stratify these patients, the duration of TKI exposure and the molecular response are important considerations.
Women who have received TKI therapy for less than 3 years or who have failed to achieve CCyR or MMR even after 3 years of treatment, such as our patient, have a higher risk of loss of CHR upon TKI discontinuation. The prime consideration in these patients should be the leukemic burden. The most straightforward management is to delay pregnancy and continue TKI therapy in the pursuit of deeper responses. If the patient is on imatinib, this could be switched to a more potent TKI. If this is not feasible due to patient preference, then once pregnancy is confirmed the TKI must be stopped and the patient managed similarly to women diagnosed in pregnancy.
A third option is assisted conception, which may be particularly relevant in older women concerned about age-related fertility loss. Depending on personal circumstances and the consent of their partner, these women can be considered for ovarian hyperstimulation, embryo creation, and subsequent embryo implantation in order to reduce the time off TKIs. Women without partners can be offered oocyte or ovarian cryopreservation. Strategies such as TKI holidays, in which highly motivated patients with regular cycles discontinue their TKI after menstruation, perform a pregnancy test 5 days post the expected ovulation, and resume their TKI if negative, are theoretically possible but carry a risk of disease progression and cannot be routinely recommended.
For women in MMR but not deep molecular remission, previous guidelines recommended that those who had sustained MMR for more than 12 months could safely discontinue their TKI and subsequently regain the same disease control after restarting.7 Table 3 summarizes the studies reporting disease control following TKI discontinuation for pregnancy. These all demonstrated that while a significant proportion of patients lose MMR upon TKI discontinuation, their original response can be regained in the majority following TKI resumption.40-43 Furthermore, Lee et al demonstrated, importantly, that almost half of those who lost MMR retained CCyR and could be managed without intervention throughout pregnancy.44
In any of these scenarios, once conception is confirmed, TKI therapy should be discontinued immediately. There is no need for increased imaging surveillance if no abnormalities are noted at the first routine ultrasound. Those in CCyR should have transcript levels evaluated every 4 to 6 weeks, whereas those with less deep responses should be monitored as appropriate for their individual level of disease control. Management is similar to that of patients diagnosed in pregnancy.
A loss of disease control can be managed in a manner similar to those described previously: utilization of IFN-α, therapeutic leukapheresis, and the consideration of TKI use in later pregnancy.
Conclusion
Pregnancy and CML can now be successfully managed in unison with minimal risk to both mother and child. A significant proportion of patients can be managed by observation only, and disease control can be achieved after starting or restarting TKI therapy. If active treatment is required, IFN-α can be used in any trimester with minimal risk to the fetus. More recently, the safe administration of TKIs in the later stages of pregnancy was reported. Most importantly, a multidisciplinary approach should be employed to provide comprehensible and succinct advice to empower both mother and family in the shared decision-making process.
Acknowledgment
Jane F. Apperley and Harry F. Robertson acknowledge the support of the National Institute of Health Research Imperial Biomedical Research Center.
Conflict-of-interest disclosure
Harry F. Robertson: no competing financial interests to declare.
Jane F. Apperley: advisory board member: Incyte, Novartis; research funding: Incyte, Pfizer; speakers bureau: Incyte, Novartis.
Off-label drug use
Harry F. Robertson: nothing to disclose.
Jane F. Apperley: nothing to disclose.