Abstract
Allogeneic bone marrow transplantation (allo-BMT) or stem cell transplantation has the potential to cure a significant proportion of patients with otherwise fatal diseases. At present, immediate survival is no longer the sole concern after allo-BMT, because many patients can survive the acute complications of the procedure and remain free of their original disease for several years. Although long-term allo-BMT survivors generally enjoy good health, for many others cure or control of the underlying disease is not accompanied by full restoration of health. The long-term physiologic effects after allo-BMT include nonmalignant organ or tissue dysfunction; changes in quality of life; infections related to delayed, or abnormal, immune reconstitution; and secondary cancers. These long-term complications and the features of chronic graft-versus-host disease (GVHD) symptoms are heterogeneous in nature, time of onset, duration, and severity. The underlying origin of these complications is often multifactorial, with chronic GVHD being the most challenging risk factor. The main aims of this review are to present transplant physicians and health care providers with an overview of these malignant and nonmalignant late complications, with a special focus on chronic GVHD. A close partnership between the transplant center, organ-specific specialties, and local primary care providers is a key component of preventive medicine. The patient can play a major role through engagement in health maintenance behaviors.
Allogenic bone marrow transplantation (allo-BMT) is an effective and curative treatment for various types of malignant and nonmalignant diseases. Many patients have now been followed for two or three decades posttransplant and are presumed to be cured. Initially limited to patients who had an HLA-identical sibling donor, allo-BMT is now an option for many more patients, because stem cells can also be obtained from HLA-matched or mismatched unrelated adult donors and from cord blood. As a result, the annual number of allo-BMT procedures has increased dramatically over time, and the number of diseases for which allo-BMT is considered appropriate has also expanded.1 Indeed, with technological advances in supportive care, histocompatibility testing, conditioning regimens, and control of graft-versus-host disease (GVHD), growth is likely to continue. It is not unreasonable to expect outcomes to improve steadily, and, consequently, increasing numbers of transplant survivors will be facing life after the initial transplant experience. At present, immediate survival is no longer the sole concern after allo-BMT, because many allo-BMT patients can survive the acute complications of the procedure and remain free of their original disease for several years.
Although long-term allo-BMT survivors generally enjoy good health, for many others cure or control of the underlying disease is not accompanied by full restoration of health.2 Moreover, many survivors are no longer under the care of transplant centers, and many community health care providers may be unfamiliar with some specific complications relevant to allo-BMT. Indeed, long-term physiologic effects after allo-BMT include nonmalignant organ or tissue dysfunction, changes in quality of life (QOL), infections related to delayed, or abnormal immune reconstitution, and secondary cancers. Many of these can be attributed to the deleterious effects of chronic GVHD. Some of these “late” consequences can start as early as 3 months after transplant, whereas others will become apparent only years or even decades later. Among the transplant community, it is common to define as late complications all events occurring beyond 3 months after allo-BMT, and separate them into delayed (3 months-2 years), late (2–10 years), and very late events (> 10 years).3
The risk and the type of complication depend on the preparative regimen received prior to allo-BMT, the age of the patient at time of allo-BMT, the presence of comorbid conditions, and the time between the treatment and follow-up. Despite an ever-growing knowledge of the natural history of the side effects of allo-BMT, long-term complications and the features of chronic GVHD symptoms are heterogeneous in nature, time of onset, duration, and severity. The latter parameters may depend on the intensity of the conditioning regimen and immunosuppressive therapies used. Theoretically, any organ can be the target of a late complication after allo-BMT, and frequently multiple causes are involved. The main aims of this review are to present transplant physicians and health care providers with an overview of these malignant and nonmalignant late complications, with a special focus on chronic GVHD. Recommended screening and preventive practices were published elsewhere and will not be discussed in this review.4 Also, this review will not address specific complications encountered in the pediatric allo-BMT population, but comprehensive description and guidelines for follow-up of pediatric allo-BMT survivors developed by the Children's Oncology Group can be found at http://www.survivorshipguidelines.org.
Chronic GVHD and Immune Deficiency
Chronic GVHD is one of the most serious consequences of allo-BMT. Too many human, emotional, societal, financial, and intellectual resources are invested in an allo-BMT procedure to consider chronic GVHD as an acceptable side effect of therapy for malignant or nonmalignant disease.
Incidence of Chronic GVHD.
Chronic GVHD is a relatively common complication, with several series reporting incidences of 40% to 70%.5,6 Whereas the prophylactic use of multiagent immunosuppression has reduced the incidence and severity of acute GVHD, the incidence of chronic GVHD is likely to increase in the future, secondary to the increasing use of allo-BMT in older patients.5 Much of this is related to the introduction of the so-called reduced-intensity conditioning (RIC) regimens more than a decade ago, more commonly used in the elderly and more likely to require donor lymphocyte infusion (DLI).
Chronic GVHD can be classified according to type of onset, need for systemic immunosuppressive therapy, or mortality risk. Based on the type of onset, chronic GVHD may evolve directly from acute GVHD (progressive), which has a poor prognosis, or may follow a period of resolution (quiescent). Finally, patients may develop chronic GVHD with no history of prior acute GVHD (de novo). Chronic GVHD and its associated immune deficiency state have been identified as the leading cause of nonrelapse mortality (NRM) in allo-BMT survivors.7 A large registry-based study demonstrated that acute myeloid leukemia patients with active chronic GVHD at 2 years were three times more likely to experience NRM than were those without chronic GVHD and 1.7 times more likely to die from any cause.8 The primary cause of NRM associated with chronic GVHD is infection, but several studies have also demonstrated an association between chronic GVHD and reduced Karnofsky performance scores, poorer QOL, and later return to work.7,9 The Bone Marrow Transplant Survivor Study examined 584 individuals who had undergone allo-SCT between 1976 and 1999, and who survived two or more years and completed a 255-item health questionnaire. The incidence of chronic GVHD in participants was 54%, of whom 46% reported active chronic GVHD. In multivariable analyses, subjects with active chronic GVHD were more likely to report adverse general health, mental health, functional impairments, activity limitation, and pain than those with no history of chronic GVHD. However, health status did not differ between those with resolved chronic GVHD and those who never had chronic GVHD, suggesting that active chronic GVHD has a significant impact on many aspects of the overall health status of allo-SCT survivors and that, most importantly, those successfully treated for chronic GVHD do not appear to have long-term impairments.10
Clinical Risk Factors and Prevention of Chronic GVHD.
A number of patient, donor, graft, and transplant-related risk factors have been consistently associated with the onset of chronic GVHD,7 including older patient age, history of acute GVHD, female donor for male patient, certain underlying diagnoses (eg, chronic myelogenous leukemia or aplastic anemia), the use of mismatched or unrelated donors, infusion of donor lymphocytes, use of peripheral blood stem cells instead of bone marrow, and lack of T-cell depletion. More controversial risk factors for chronic GVHD include cytomegalovirus seropositivity or reactivation, previous splenectomy, steroid prophylaxis for acute GVHD, and high CD34+ cell count in the graft.11 On the other hand, recipients of unrelated cord blood transplants are likely at lower risk for chronic GVHD. Efforts to prevent acute GVHD have generally not resulted in a significant decrease in the incidence of chronic GVHD. Nonetheless, in pursuing preventive strategies, it is important to recognize that, in allo-BMT for malignant disease, chronic GVHD may be also associated with a beneficial graft-versus-tumor effect. However, evidence indicates that increased severity of chronic GVHD does not necessarily correlate with an additive benefit of graft-versus-tumor,12 so the main focus should remain the prevention of chronic GVHD. Unfortunately, many specific attempts to decrease the incidence of chronic GVHD by preemptive treatment have failed thus far. For instance, extending the time period of cyclosporine immunosuppression produced equivocal results.13 Another strategy has been to focus only on selected patient populations that are at high risk of developing severe chronic GVHD. The addition of antithymocyte globulin to cyclosporine and methotrexate provided significant protection against extensive chronic GVHD and chronic lung dysfunction, reduced late transplant mortality, and improved the QOL in patients undergoing unrelated donor transplantation.14,15
Clinical Manifestations of Chronic GVHD.
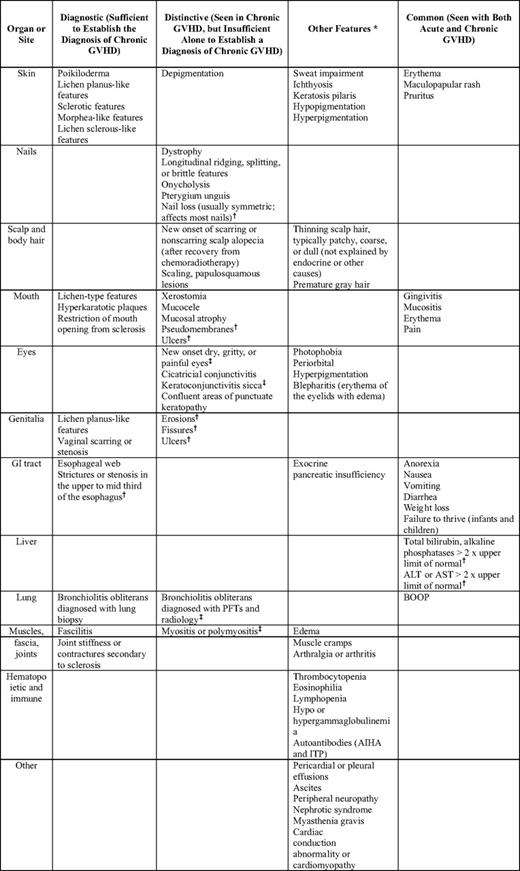
The list of clinical manifestations characteristic of chronic GVHD is given in Table 1 and closely resemble those of several well-recognized autoimmune syndromes, particularly systemic sclerosis, but also Sjogren's syndrome, primary biliary cirrhosis, lichen planus, wasting syndrome, bronchiolitis obliterans, myositis, and others.16 The most commonly involved organs are skin (65%–80%), mouth (48%–72%), liver (40%–73%), and eyes (18%–47%). Debilitation, joint contractures, and profound immunosuppression with recurrent bacterial and other infections are prominent characteristics of untreated or inadequately treated chronic GVHD.17 The median time to onset of chronic GVHD is approximately 6 months after transplant, and most cases manifest by 2 years posttransplant. The prevalence of chronic GVHD starts dropping 2 to 3 years after transplant, but even at 5 years, up to 20% of patents have symptoms requiring systemic immunosuppressive therapy.17 Although in most cases, chronic GVHD ultimately resolves, in a proportion of patients, irreversible changes continue to significantly impact QOL (eg, advanced sicca syndrome, bronchiolitis obliterans, or skin contractures). Manifestations characteristic of chronic GVHD can also begin early after allo-BMT, even before day 100 posttransplant, and manifestations that are typical for acute GVHD can persist long after day 100. This chronological overlap of acute and chronic GVHD onset is especially common today, with the increasing use of the so-called nonmyeloablative or RIC regimens and administration of donor lymphocyte infusion.18 For this reason, the differential diagnosis between acute and chronic GVHD cannot be made solely based on the time interval posttransplant and must adhere to the National Institutes of Health criteria.19
Immune Deficiency and Chronic GVHD.
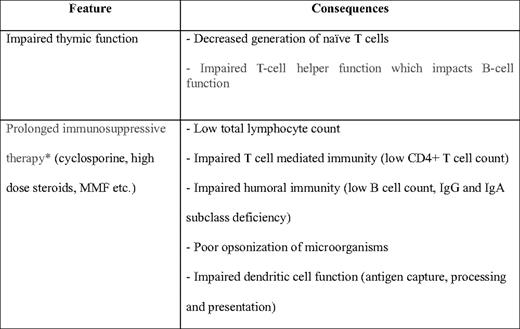
Immune recovery plays a pivotal role in recovery after allo-BMT. Variables related to patient or transplant characteristics (eg, age of recipient, stem cell source and engineering, type and duration of the underlying disease and the conditioning regimen) may influence the recovery of functional immunity. Nevertheless, chronic GVHD and the consequent administration of systemic immunosuppressive drugs are the major factors affecting immune reconstitution of both innate and adaptive immunity, and the degree of immunosuppression experienced by individual patients varies greatly. Moreover, it remains to be seen whether long-term survivors who have developed severe chronic GVHD are able to recover normal immune function posttransplant. Donor source (marrow vs peripheral blood vs cord blood), and the degree of HLA compatibility between donor and recipient also affect the pace of immune reconstitution. Persistently low B-cell counts, an inverted CD4/CD8 ratio, and a decreased synthesis of immunoglobulins (Ig) are all risk factors associated with late infections.20 Thymic recovery after transplantation may be an important factor in long-term return to full immunologic function.21 B cells are decreased in numbers for up to 12 months, whereas Ig levels usually show an initial fall, followed by recovery within months (for IgG and IgM) to years (for IgA). This finding parallels the pattern seen in B-cell ontogeny and may reflect the failure of posttransplant B cells to receive or respond to the T-cell help involved in the isotype switching.22 Factors contributing to immune deficiency in the context of chronic GVHD are summarized in Table 2.
Infections and Chronic GVHD.
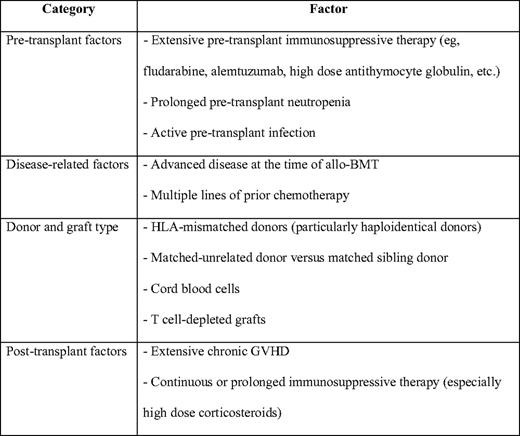
Late infectious complications after allo-BMT have been extensively reviewed in recent years, and updated guidelines for preventing and treating these opportunistic infections have been recently published.23 Factors affecting the risk of late infections after allo-BMT are summarized in Table 3. However, one must acknowledge that this is a rapidly moving field because significant changes have occurred in more recent years. These changes include new antimicrobial agents (especially antifungal agents),24 wider use of RIC, the increasing age of allo-BMT recipients, and more frequent use of alternative donor stem cell sources (eg, haploidentical donors and umbilical cord blood), all of which are associated with significantly delayed immune reconstitution.25 Unfortunately, there is currently no definitive marker of immune reconstitution that would predict long-term infectious risk after allo-BMT. Despite these important advances, infections still occur with increased frequency or severity among allo-BMT recipients. Briefly, susceptibility to encapsulated bacteria (Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis) has been well documented in patients with ongoing or previous chronic GVHD. Late fungal or viral infections (eg, cytomegalovirus) almost invariably occur in patients with active chronic GVHD requiring ongoing corticosteroids. On the other hand, Varicella zoster can occur frequently in patients with or without GVHD after acyclovir prophylaxis has been discontinued. Finally, late Pneumocystis jiroveci pneumonia and Toxoplasma gondii infections are more common in patients receiving active treatment for chronic GVHD, and prophylaxis with trimethoprimsulfamethoxazole should be continued for several months after the cessation of systemic immunosuppressive therapy, given the long-lasting immune defects characteristic of chronic GVHD.26
Nonmalignant Late Effects After Allo-BMT
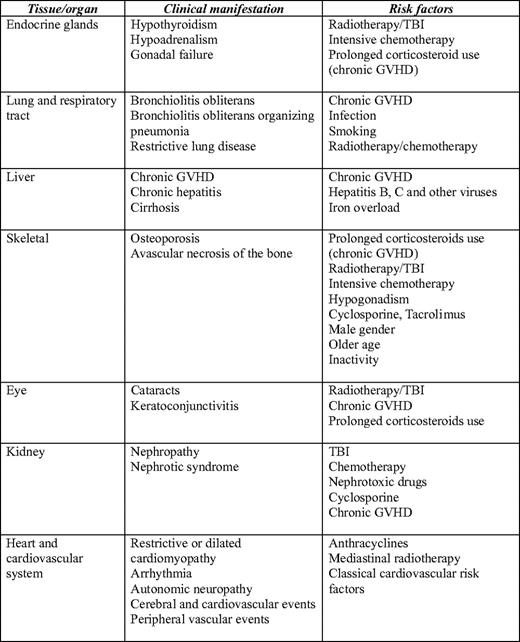
Table 4 summarizes the most important and frequent nonmalignant late effects occurring in adults after allo-BMT and their risk factors. Common dimensions of health-related QOL and psychosocial outcomes across the trajectory of allo-BMT are discussed in “Quality of Life and Psychosocial Issues with Allogeneic BMT” in this volume.
Endocrine Dysfunction.
There is a high risk of pituitary, gonadal, thyroid, and adrenal dysfunctions among transplant survivors. Multiple endocrine abnormalities may occur, especially after total body irradiation (TBI)-containing regimens, but patients after high-dose cytotoxic agents are also not exempt. Thyroid dysfunction was recognized early as one of the most frequent late complications of allo-BMT, and depends mainly on the cumulative irradiation dose and the time from exposure. Seven percent to 15% of transplant patients develop subclinical hypothyroidism.27 A higher incidence is observed after single-dose TBI rather than fractionated-dose TBI and conditioning without irradiation. The onset of thyroid organ dysfunction occurs usually around 5 years after irradiation, but may occur much sooner or later.
Hypoadrenalism may occur in patients on prolonged corticosteroid therapy for GVHD treatment. Gradual tapering of corticosteroids is appropriate. For patients requiring surgical procedures or with acute medical illnesses, short-term “stress” replacement is warranted. Gonadal function is impaired lifelong in the majority of patients receiving standard myeloablative conditioning prior to allo-BMT. The major cause of gonadal damage leading to hypergonadotropic hypogonadism is irradiation.28 Similar damage can also be caused by busulfan, whereas cyclophosphamide is usually associated with only minor effects on gonadal function.29 The ovaries are usually more vulnerable to TBI and chemotherapy than the testes (although this may depend on age and dose of TBI), and hypergonadotropic hypogonadism is very frequent.
Fertility Following Allo-BMT.
Lifelong infertility is typical, but not universal after allo-BMT. The exact incidence of fertility following allo-BMT is difficult to establish, but the overall incidence of conception is rather low.30,31 There are some confounding factors that preclude accurately predicting the features of fertility after allo-BMT, because many patients of child-bearing age have already completed their families and/or do not wish to become parents following the diagnosis of a malignant disease. Some studies have suggested late recovery of spermatogenesis in a minority of men (10%–15%), and ovarian recovery has been observed in some women (5%–10%). Return of gonadal function following conditioning with cyclophosphamide only for severe aplastic anemia was noted in more than 50% of adult female survivors, and 27% of women subsequently conceived.32 Similarly, 61% of adult male survivors of transplant for aplasia had return of sperm production and 26% subsequently fathered children. In thalassemic patients, gonadal failure is common as a result of both transfusional hemosiderosis and the busulfan-based conditioning regimen, and pregnancies are very rare. In patients transplanted for malignant diseases receiving TBI-based conditioning, gonadal failure is the rule. Recovery of gonadal function occurs in 10% to 14% of the women, where it is closely associated with young age at transplant, and in less than 20% of men. There have been no pregnancies reported using chemotherapy-based conditioning (busulphan and cyclophosphamide) for women with leukemia, whereas a few men have subsequently fathered children naturally. Melphalan alone or in combination with etoposide or cyclophosphamide in the conditioning regimen is compatible with return of fertility in up to 50% of cases.29 Nevertheless, one should bear in mind that the picture may evolve in the next few years with the advent of RIC transplants, especially in younger females. Also, the putative lower risk of infertility in younger women after RIC brings also a new risk of unwanted pregnancy and issues of contraception counseling.
Lung and Respiratory Tract Late Effects.
Significant late toxicity involving both the airways and lung parenchyma affects at least 15% to 40% of patients after allo-BMT.33 Lung injury from the cytotoxic agents in the conditioning regimen has become much less frequent today, but can lead to pulmonary interstitial fibrosis. Late interstitial pneumonitis occurs infrequently, but more often in patients with chronic GVHD. Restrictive lung disease is frequently observed 3 to 6 months after stem cell tranplantation in patients conditioned with TBI, although some patients develop severe late restrictive defects.34
The most common noninfectious late complications include bronchiolitis obliterans (BO), BO organizing pneumonia, and idiopathic pneumonia syndrome. Chronic obstructive pulmonary disease can be detected in up to 20% of long-term survivors after allo-BMT. When chronic GVHD affects the lung tissue, the result is invariably the BO syndrome, which is characterized by a nonspecific inflammatory injury affecting primarily the small airways. Recent data suggest that BO may affect up to 6% of allo-BMT recipients and dramatically alter survival, with overall survival of only 13% at 5 years.35 BO is strongly associated with chronic GVHD, which is likely responsible for the initial epithelial injury to the small airways, with further damage caused by recurrent infections. Consequently, infections or unexplained deterioration should be aggressively investigated and treated appropriately.36 In this perspective, it is important to mention the insufficiency of current guidelines relative to early diagnosis of BO syndrome. As of now, these guidelines recommend PFTs at 12 months post transplant and are in the discrepancy with the cGVHD specific prevention guidelines which advise pulmonary function test screening every 3 months during the first year posttransplant. Because BO syndrome is an insidious process and cases rapidly progressing during the first year posttransplant have worst prognosis, regular early pulmonary function tests are currently the only strategy for potential early intervention.
Liver Late Effects.
Liver involvement by chronic GVHD is the most common cause of late hepatic disease. However, several causes of liver disease may coexist. Although the risk of acquiring hepatitis B virus or hepatitis C virus (HCV) infection from blood transfusion is currently greatly reduced, chronic hepatitis from hepatitis B virus or HCV can occur due to transmission via the graft or from transfusion support. The prevalence of “de novo” infection in patients receiving hepatitis B surface antigen (HBsAg) and HCV RNA– transplants is around 2.0% and 7.4%, respectively. The prevalence of donors positive for HBsAg and HCV RNA, is around 2.6% and 3.6%, respectively.37 Although patients with chronic hepatitis B virus or HCV, generally show mild-to-moderate liver disease on long-term follow-up, progression to cirrhosis can occur and may represent an important clinical problem in very long-term allo-BMT survivors. Other viruses—such as the herpesviruses (including cytomegalovirus), adenoviruses, and Epstein-Barr virus—may be also implicated. Iron overload from transfusions or altered iron absorption can be observed in long-term allo-BMT survivors.38 In heavily transfused patients, iron can also worsen the natural course of chronic hepatitis, and contribute to liver fibrosis, cirrhosis, and hepatocellular carcinoma, as well as to cardiac dysfunction. Finally, iron overload increases the risk of opportunistic infections, especially in immunocompromised patients.39
Late Skeletal Disorders.
In the long term, allo-BMT can induce bone loss and osteoporosis via the toxic effects of TBI, chemotherapy, or other drug therapy and hypogonadism. The cumulative dose and durations of glucocorticoid therapy and cyclosporine or tacrolimus therapy showed significant associations with loss of bone marrow density, with nontraumatic fractures occurring in around 10% of patients.40 The incidence of avascular necrosis of bone varies from 5% to 15%, and is diagnosed at a mean time of 18 months after allo-BMT. Risk factors for avascular necrosis include mainly steroids (both total dose and duration) and high-dose TBI.41,42
Late Ophthalmologic Side Effects.
Late ocular complications of both the posterior and anterior segments can occur after allo-BMT.43 Complications of the posterior segment include microvascular retinopathy, optic disk edema, hemorrhagic complications, and infectious retinitis. Microvascular retinopathy occurs mainly after the use of TBI and/or cyclosporine. Ischemic retinopathy has been reported in patients conditioned with busulfan and cyclophosphamide without irradiation, but it is likely that the development of ischemic eye lesions is a multifactorial process leading to capillary damage of the fundus.
The two most common late complications affecting the anterior segment are cataract formation and keratoconjunctivitis sicca syndrome. Cataracts can occur within 3 to 4 years, and the incidence may reach more than 80% at 6 to 10 years posttransplant. The use of TBI (particularly single fraction), steroid treatment for longer than 3 months, and older age are well-recognized risk factors for cataract development.44 Keratoconjunctivitis sicca is most commonly a manifestation of chronic GVHD and is usually part of a more general syndrome with xerostomia, vaginitis, and dryness of the skin, but can also occur occasionally in the absence of GVHD. The incidence of late-onset keratoconjunctivitis sicca syndrome reaches nearly 40% in patients with chronic GVHD, compared with less than 10% in those without GVHD.45
Late Renal and Cardiovascular Complications.
Little is known about the magnitude of late renal dysfunction after allo-BMT. The use of nephrotoxic agents (chemotherapy prior to allo-BMT, the conditioning regimen, and antiinfectious and immunosuppressive agents), older age, female gender, hypertension after allo-BMT, low pretransplant glomerular filtration rate, the use of fludarabine, and the use of single-dose TBI have all been reported to increase the risk of chronic kidney disease, defined as a sustained decrease in glomerular filtration rate below levels of 60 mL/min/1.73 m2.46 Using this definition, the cumulative incidence at 10 years is approximately 27%.47 However, only a minority of allo-BMT patients will experience severe kidney disease requiring chronic dialysis.46 The diagnostic pathologic features include tubular atrophy, interstitial fibrosis, and calcineurin inhibitor arteriolopathy. Nephrotic syndrome has been observed in a few patients and can be now considered as a renal complication of chronic GVHD that responds to corticosteroids.48 Antibody-producing residual host B cells persisting after RIC allo-BMT might predispose to a membranous nephropathy resulting in nephrotic syndrome.49
Although data on long-term cardiac complications after allo-BMT are scarce, long-term survivors of allo-BMT are at risk for a variety of cardiac and cardiovascular late effects. Late cardiotoxicity includes cardiomyopathy, congestive heart failure, valvular dysfunction, or arrhythmia, with the total cumulative dose of anthracyclines being the main cause of cardiomyopathy. Mediastinal radiotherapy and subsequent fibrosis can contribute to the onset of restrictive cardiomyopathy and induce arrhythmias, autonomic dysfunction, and valvular defects. Compared with a general population, the risk of late death due to cardiac complications is 2.3-fold higher after allo-BMT.50 However, one should consider these figures with caution, because cardiac complications will occur decades after treatment as very late events.51
In terms of late cardiovascular complications, several cases of young patients (all of whom had chronic GVHD) developing fatal stroke or coronary artery disease have been reported.52 In a recent study, the cumulative incidence of an arterial event (eg, cerebrovascular disease, coronary artery disease, or peripheral artery disease after allo-BMT) was 22% at 25 years. When adjusted for age, patients from this series had a 7-fold increased relative risk of an arterial event at 15 years.51 In the European Group for Blood and Marrow Transplantation registry, the cumulative incidence of an arterial event at 15 years was 6%.3 The link between cardiovascular events after allo-BMT and chronic GVHD may be related to the decreased numbers of microvessels in the subcutaneous compartment and to endothelial injury.53 Finally, these late cardiovascular events are likely favored by other cardiovascular risk factors, such as diabetes, hypertriglyceridemia, low levels of high-density lipoprotein cholesterol, endocrine dysfunction, hypertension, and obesity.51
Late Secondary Malignancies After Allo-BMT
TBI and the chemotherapeutic drugs used prior to allo-BMT and as part of the conditioning regimen can induce new secondary malignancies after allo-BMT. This is attributed to the mutagenic risk of irradiation and chemotherapy, the genetic predisposition of the patient to develop cancer, prolonged immunosuppression, and, in elderly patients, to age-related risk. Such secondary malignancies can fall into three categories: (1) solid tumors, (2) hematologic malignancies (mainly poor prognosis therapy-related leukemias), and (3) posttransplant lymphoproliferative disorder. Secondary leukemias occur earlier than solid tumors, with a peak occurrence at 2 to 6 years after allo-BMT, whereas solid cancers (melanoma, liver, brain, bone, breast, connective tissue, squamous cell cancers of the buccal cavity, and skin) are diagnosed later.54,55 Allo-BMT patients develop new solid cancers at twice the rate expected based on general population rates (observed-to-expected ratio 2:1), with the risk increasing over time. Moreover, the risk reached three-fold among patients followed for 15 years or more after transplantation. In another series, the incidence of solid tumors was around 3.5% at 10 years and 12.8% at 15 years.56 New findings from a large, more recent series showed a lower incidence of solid tumors and that the risk of developing a nonsquamous cell carcinoma following conditioning radiation was highly dependent on age at exposure.57
Conclusions
Allo-BMT has the potential to cure a significant proportion of patients with otherwise fatal diseases. Improved short-term survival exposes patients to long-term complications and side effects. All of these late complications present with a great diversity in respect of frequency, time of onset, risk factors, prevention and treatment approaches, and outcome. The underlying origin of these complications is often multifactorial, with chronic GVHD being the most challenging risk factor. A preventable death with a functioning hematopoietic allograft is not a marker of success. The long-term goal is maintenance of health and to ensure the best possible QOL. A close partnership between the transplant center, organ-specific specialties, and local primary care providers is a key component of preventive medicine toward screening and treating deleterious long-term side effects lifelong after allo-BMT. Long-term follow-up teams already exist within the biggest transplant programs worldwide, but the optimal care model is yet to be defined and has to be adapted to local constraints. The patient can play a major role through engagement in health maintenance behaviors.
Acknowledgments
M.M. would like to dedicate this review to the memory of “Rabab.” Several relevant reports and publications could not be included in the present review. We would like to apologize for those colleagues whose work could not be cited because of space limitation as per the American Society of Hematology requirements.
M.M. acknowledges the support of the “Région Pays de Loire,” the “Association pour la Recherche sur le Cancer (ARC),” the “Fondation de France,” the “Fondation contre la Leucémie,” the “Agence de Biomédecine,” the “Association Cent pour Sang la Vie,” and the “Association Laurette Fuguain,” for their generous and continuous support for his clinical and basic research work.
J.F.A. acknowledges the support of the National Institute for Health Research Biomedical Research Centre.
Disclosures
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Off-label drug use: None disclosed.
Correspondence
Mohamad Mohty, MD, PhD, Hématologie Clinique, CHU de Nantes, Place A. Ricordeau, F-44093 Nantes Cedex, France; Phone: +33 240 083271; Fax: +33 240 083250; e-mail: mohamad.mohty@univ-nantes.fr